Amanda Bingaman, Rohan V Gupta, Srinivasa P Kanuparthi, Bong-Soo Kim
{"title":"前后路联合内固定融合术治疗椎体骨髓炎后严重颈椎后凸和冠状畸形1例并文献复习。","authors":"Amanda Bingaman, Rohan V Gupta, Srinivasa P Kanuparthi, Bong-Soo Kim","doi":"10.21037/jss-24-133","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vertebral osteomyelitis (VO) can cause devastating neurological injury when there is a failure in early identification or prompt initiation of targeted antimicrobial therapy. Surgery is indicated for severe cases, such as those with a pathologic fracture or deformity producing spinal instability, or epidural abscess causing severe spinal cord compression with new neurologic deficit. A delayed severe combined kyphotic and coronal cervical deformity after cervical decompression is rare, and appropriate surgical management requires careful selection of approach and intraoperative technique.</p><p><strong>Case description: </strong>We present a medically complex 58-year-old male who developed a severe combined kyphotic and coronal cervical deformity in a delayed fashion after an initial posterior cervical decompression for symptomatic epidural abscess associated with VO. The patient underwent a combined two-stage anterior and posterior approach. The patient tolerated both surgeries without complication and follow-up imaging demonstrated correction of cervical sagittal and coronal alignment. Interestingly, despite appropriate antibiotic therapy, intraoperative culture during deformity correction yielded growth of the initial culprit microorganism.</p><p><strong>Conclusions: </strong>A two-stage anterior and posterior approach with multi-level anterior cervical decompression and instrumented fusion followed by posterior cervicothoracic instrumented fusion addresses the primary surgical goals of affected spinal segment decompression, restoration of appropriate spinal alignment, and prevention of further deformity or neurologic compromise. This report highlights suitability of techniques accessible to most spinal surgeons for correction of a multiplanar deformity, contributes to the ongoing discussion regarding instrumentation in the setting of an active spinal infection, and emphasizes the importance of close clinical and radiographic follow-up in this patient population.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"11 2","pages":"363-370"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226177/pdf/","citationCount":"0","resultStr":"{\"title\":\"Combined anterior and posterior instrumented fusion for correction of severe cervical kyphotic and coronal deformity in vertebral osteomyelitis: a case report with literature review.\",\"authors\":\"Amanda Bingaman, Rohan V Gupta, Srinivasa P Kanuparthi, Bong-Soo Kim\",\"doi\":\"10.21037/jss-24-133\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Vertebral osteomyelitis (VO) can cause devastating neurological injury when there is a failure in early identification or prompt initiation of targeted antimicrobial therapy. Surgery is indicated for severe cases, such as those with a pathologic fracture or deformity producing spinal instability, or epidural abscess causing severe spinal cord compression with new neurologic deficit. A delayed severe combined kyphotic and coronal cervical deformity after cervical decompression is rare, and appropriate surgical management requires careful selection of approach and intraoperative technique.</p><p><strong>Case description: </strong>We present a medically complex 58-year-old male who developed a severe combined kyphotic and coronal cervical deformity in a delayed fashion after an initial posterior cervical decompression for symptomatic epidural abscess associated with VO. The patient underwent a combined two-stage anterior and posterior approach. The patient tolerated both surgeries without complication and follow-up imaging demonstrated correction of cervical sagittal and coronal alignment. Interestingly, despite appropriate antibiotic therapy, intraoperative culture during deformity correction yielded growth of the initial culprit microorganism.</p><p><strong>Conclusions: </strong>A two-stage anterior and posterior approach with multi-level anterior cervical decompression and instrumented fusion followed by posterior cervicothoracic instrumented fusion addresses the primary surgical goals of affected spinal segment decompression, restoration of appropriate spinal alignment, and prevention of further deformity or neurologic compromise. This report highlights suitability of techniques accessible to most spinal surgeons for correction of a multiplanar deformity, contributes to the ongoing discussion regarding instrumentation in the setting of an active spinal infection, and emphasizes the importance of close clinical and radiographic follow-up in this patient population.</p>\",\"PeriodicalId\":17131,\"journal\":{\"name\":\"Journal of spine surgery\",\"volume\":\"11 2\",\"pages\":\"363-370\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226177/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of spine surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/jss-24-133\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-133","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Combined anterior and posterior instrumented fusion for correction of severe cervical kyphotic and coronal deformity in vertebral osteomyelitis: a case report with literature review.
Background: Vertebral osteomyelitis (VO) can cause devastating neurological injury when there is a failure in early identification or prompt initiation of targeted antimicrobial therapy. Surgery is indicated for severe cases, such as those with a pathologic fracture or deformity producing spinal instability, or epidural abscess causing severe spinal cord compression with new neurologic deficit. A delayed severe combined kyphotic and coronal cervical deformity after cervical decompression is rare, and appropriate surgical management requires careful selection of approach and intraoperative technique.
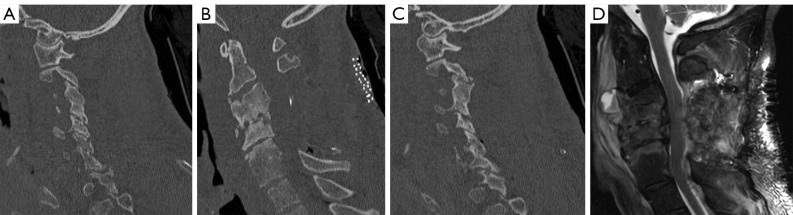
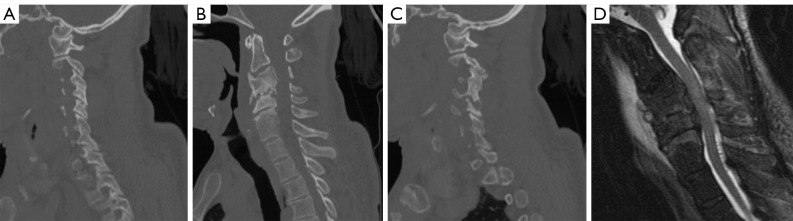
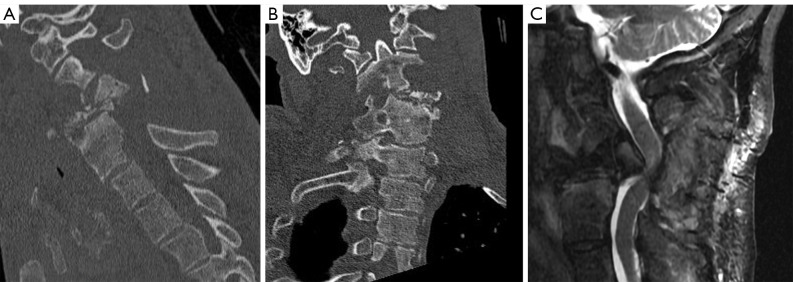
Case description: We present a medically complex 58-year-old male who developed a severe combined kyphotic and coronal cervical deformity in a delayed fashion after an initial posterior cervical decompression for symptomatic epidural abscess associated with VO. The patient underwent a combined two-stage anterior and posterior approach. The patient tolerated both surgeries without complication and follow-up imaging demonstrated correction of cervical sagittal and coronal alignment. Interestingly, despite appropriate antibiotic therapy, intraoperative culture during deformity correction yielded growth of the initial culprit microorganism.
Conclusions: A two-stage anterior and posterior approach with multi-level anterior cervical decompression and instrumented fusion followed by posterior cervicothoracic instrumented fusion addresses the primary surgical goals of affected spinal segment decompression, restoration of appropriate spinal alignment, and prevention of further deformity or neurologic compromise. This report highlights suitability of techniques accessible to most spinal surgeons for correction of a multiplanar deformity, contributes to the ongoing discussion regarding instrumentation in the setting of an active spinal infection, and emphasizes the importance of close clinical and radiographic follow-up in this patient population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


