Keke Chen, Yuli Zhu, Han Liu, Minying Deng, Wentao Kong, Wenping Wang
{"title":"基于多模式影像和临床指标的一种罕见且高度侵袭性的肝细胞癌亚型的术前预测。","authors":"Keke Chen, Yuli Zhu, Han Liu, Minying Deng, Wentao Kong, Wenping Wang","doi":"10.2147/JHC.S533963","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To develop and validate a reliable preoperative non-invasive diagnostic model for dual-phenotype hepatocellular carcinoma (DPHCC) by integrating multimodal imaging and clinical indicators, thereby facilitating clinical decision-making.</p><p><strong>Patients and methods: </strong>222 pathologically confirmed patients (61 with DPHCC, 161 with non-DPHCC) were retrospectively enrolled in this study and randomly assigned to training and validation cohorts in an 8:2 ratio. Serological and multimodal imaging characteristics were analyzed. Univariate and multivariate logistic regression analyses identified independent DPHCC predictors and built a nomogram. Model performance and clinical utility were assessed by receiver operating characteristic (ROC) and decision curve analysis (DCA) curve respectively. The calibration curve was used to verify the model. Recurrence-free survival (RFS) was assessed using Kaplan-Meier and Log rank tests.</p><p><strong>Results: </strong>In multivariate analysis, age (OR=0.91; P < 0.001), LDH (OR=1.03; P=0.002), PT (OR=0.14; P < 0.001), AFP (OR=4.04; P=0.019), Adler grade (OR=0.17; P=0.037), non-enhancing area (OR=8.30; P=0.004), arterial phase hyperenhancement (OR=0.12; P=0.015) and enhancing capsule (OR=0.32; P=0.04) were independent predictors of DPHCC. The nomogram achieved a robust predictive performance with C-index (0.92 vs 0.87) and accuracy (0.87 vs 0.86) in the training and validation cohorts. In addition, the calibration curve and DCA also showed good model performance. DPHCC patients had significantly lower RFS than non-DPHCC patients (P = 0.037).</p><p><strong>Conclusion: </strong>A nomogram was established for non-invasive prediction of DPHCC risk utilizing multimodal imaging combined with clinical indicators to help achieve personalized treatment.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1253-1266"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227323/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative Prediction of a Rare and Highly Aggressive Subtype of Hepatocellular Carcinoma Based on Multimodal Imaging and Clinical Indicators.\",\"authors\":\"Keke Chen, Yuli Zhu, Han Liu, Minying Deng, Wentao Kong, Wenping Wang\",\"doi\":\"10.2147/JHC.S533963\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To develop and validate a reliable preoperative non-invasive diagnostic model for dual-phenotype hepatocellular carcinoma (DPHCC) by integrating multimodal imaging and clinical indicators, thereby facilitating clinical decision-making.</p><p><strong>Patients and methods: </strong>222 pathologically confirmed patients (61 with DPHCC, 161 with non-DPHCC) were retrospectively enrolled in this study and randomly assigned to training and validation cohorts in an 8:2 ratio. Serological and multimodal imaging characteristics were analyzed. Univariate and multivariate logistic regression analyses identified independent DPHCC predictors and built a nomogram. Model performance and clinical utility were assessed by receiver operating characteristic (ROC) and decision curve analysis (DCA) curve respectively. The calibration curve was used to verify the model. Recurrence-free survival (RFS) was assessed using Kaplan-Meier and Log rank tests.</p><p><strong>Results: </strong>In multivariate analysis, age (OR=0.91; P < 0.001), LDH (OR=1.03; P=0.002), PT (OR=0.14; P < 0.001), AFP (OR=4.04; P=0.019), Adler grade (OR=0.17; P=0.037), non-enhancing area (OR=8.30; P=0.004), arterial phase hyperenhancement (OR=0.12; P=0.015) and enhancing capsule (OR=0.32; P=0.04) were independent predictors of DPHCC. The nomogram achieved a robust predictive performance with C-index (0.92 vs 0.87) and accuracy (0.87 vs 0.86) in the training and validation cohorts. In addition, the calibration curve and DCA also showed good model performance. DPHCC patients had significantly lower RFS than non-DPHCC patients (P = 0.037).</p><p><strong>Conclusion: </strong>A nomogram was established for non-invasive prediction of DPHCC risk utilizing multimodal imaging combined with clinical indicators to help achieve personalized treatment.</p>\",\"PeriodicalId\":15906,\"journal\":{\"name\":\"Journal of Hepatocellular Carcinoma\",\"volume\":\"12 \",\"pages\":\"1253-1266\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227323/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hepatocellular Carcinoma\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/JHC.S533963\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S533963","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Preoperative Prediction of a Rare and Highly Aggressive Subtype of Hepatocellular Carcinoma Based on Multimodal Imaging and Clinical Indicators.
Purpose: To develop and validate a reliable preoperative non-invasive diagnostic model for dual-phenotype hepatocellular carcinoma (DPHCC) by integrating multimodal imaging and clinical indicators, thereby facilitating clinical decision-making.
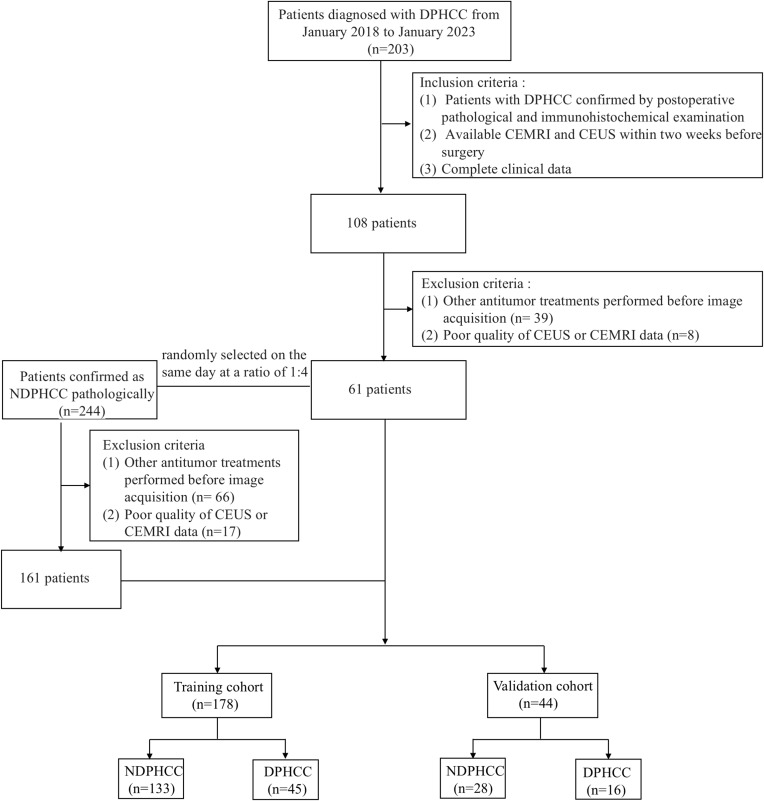
Patients and methods: 222 pathologically confirmed patients (61 with DPHCC, 161 with non-DPHCC) were retrospectively enrolled in this study and randomly assigned to training and validation cohorts in an 8:2 ratio. Serological and multimodal imaging characteristics were analyzed. Univariate and multivariate logistic regression analyses identified independent DPHCC predictors and built a nomogram. Model performance and clinical utility were assessed by receiver operating characteristic (ROC) and decision curve analysis (DCA) curve respectively. The calibration curve was used to verify the model. Recurrence-free survival (RFS) was assessed using Kaplan-Meier and Log rank tests.
Results: In multivariate analysis, age (OR=0.91; P < 0.001), LDH (OR=1.03; P=0.002), PT (OR=0.14; P < 0.001), AFP (OR=4.04; P=0.019), Adler grade (OR=0.17; P=0.037), non-enhancing area (OR=8.30; P=0.004), arterial phase hyperenhancement (OR=0.12; P=0.015) and enhancing capsule (OR=0.32; P=0.04) were independent predictors of DPHCC. The nomogram achieved a robust predictive performance with C-index (0.92 vs 0.87) and accuracy (0.87 vs 0.86) in the training and validation cohorts. In addition, the calibration curve and DCA also showed good model performance. DPHCC patients had significantly lower RFS than non-DPHCC patients (P = 0.037).
Conclusion: A nomogram was established for non-invasive prediction of DPHCC risk utilizing multimodal imaging combined with clinical indicators to help achieve personalized treatment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


