Sophie Samuel, Jalon Barnes, Lynn Yamane, Eugene Uh, Cyprian C Afunugo, Bosco Seong Kyu Yang, Huimahn Alex Choi
{"title":"早期与晚期静脉血栓栓塞的外伤性脑损伤患者的住院死亡率和出血风险","authors":"Sophie Samuel, Jalon Barnes, Lynn Yamane, Eugene Uh, Cyprian C Afunugo, Bosco Seong Kyu Yang, Huimahn Alex Choi","doi":"10.1055/a-2616-1673","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study reviewed the management and outcomes of traumatic brain injury (TBI) patients who developed venous thromboembolism (VTE) during hospitalization, focusing on the timing of VTE diagnosis and anticoagulation initiation.</p><p><strong>Methods: </strong>This retrospective, single-center study utilized data from the University of Texas Trauma Database. Patients were categorized based on VTE diagnosis timing (early ≤7 days, late >7 days). The primary outcome was in-hospital mortality. Secondary outcomes included mortality specifically among patients who were receiving anticoagulation treatment, hemorrhagic complications, predictors associated with early anticoagulation initiation (defined as ≤ 7 days from VTE diagnosis), and whether anticoagulation timing influenced mortality.</p><p><strong>Results: </strong>Among 237 patients (early: 145, late: 92), the mean age was 59 ± 20 years vs. 55 ± 20 years ( <i>p</i> = 0.133). Males comprised 68% vs. 78% ( <i>p</i> = 0.038). Subdural hematomas were the predominant injury (63% vs. 68%, <i>p</i> = 0.443). In-hospital mortality was similar (10% vs. 13%, <i>p</i> = 0.524) and did not differ between anticoagulated and non-anticoagulated patients ( <i>p</i> = 0.94). Among patients who died, 73% in the early group and 100% in the late group had received anticoagulation ( <i>p</i> = 0.053). Hemorrhage expansion was more frequent in early VTE patients (40% vs. 0%, <i>p</i> = 0.046). Pulmonary embolism was associated with early anticoagulation (OR = 1.86, 95% CI: 1.09-3.17, <i>p</i> = 0.023), while severe neurologic injury (GCS <9) reduced its likelihood (OR = 0.53, 95% CI: 0.28-0.98, <i>p</i> = 0.042).</p><p><strong>Conclusion: </strong>In-hospital mortality did not differ by VTE timing or anticoagulation status. However, hemorrhage expansion was more frequent in early VTE patients, particularly those with subdural hematomas, emphasizing the need for individualized anticoagulation strategies.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"9 ","pages":"a26161673"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12223956/pdf/","citationCount":"0","resultStr":"{\"title\":\"In-Hospital Mortality and Hemorrhagic Risks in Traumatic Brain Injury Patients with Early vs. Late Venous Thromboembolism.\",\"authors\":\"Sophie Samuel, Jalon Barnes, Lynn Yamane, Eugene Uh, Cyprian C Afunugo, Bosco Seong Kyu Yang, Huimahn Alex Choi\",\"doi\":\"10.1055/a-2616-1673\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study reviewed the management and outcomes of traumatic brain injury (TBI) patients who developed venous thromboembolism (VTE) during hospitalization, focusing on the timing of VTE diagnosis and anticoagulation initiation.</p><p><strong>Methods: </strong>This retrospective, single-center study utilized data from the University of Texas Trauma Database. Patients were categorized based on VTE diagnosis timing (early ≤7 days, late >7 days). The primary outcome was in-hospital mortality. Secondary outcomes included mortality specifically among patients who were receiving anticoagulation treatment, hemorrhagic complications, predictors associated with early anticoagulation initiation (defined as ≤ 7 days from VTE diagnosis), and whether anticoagulation timing influenced mortality.</p><p><strong>Results: </strong>Among 237 patients (early: 145, late: 92), the mean age was 59 ± 20 years vs. 55 ± 20 years ( <i>p</i> = 0.133). Males comprised 68% vs. 78% ( <i>p</i> = 0.038). Subdural hematomas were the predominant injury (63% vs. 68%, <i>p</i> = 0.443). In-hospital mortality was similar (10% vs. 13%, <i>p</i> = 0.524) and did not differ between anticoagulated and non-anticoagulated patients ( <i>p</i> = 0.94). Among patients who died, 73% in the early group and 100% in the late group had received anticoagulation ( <i>p</i> = 0.053). Hemorrhage expansion was more frequent in early VTE patients (40% vs. 0%, <i>p</i> = 0.046). Pulmonary embolism was associated with early anticoagulation (OR = 1.86, 95% CI: 1.09-3.17, <i>p</i> = 0.023), while severe neurologic injury (GCS <9) reduced its likelihood (OR = 0.53, 95% CI: 0.28-0.98, <i>p</i> = 0.042).</p><p><strong>Conclusion: </strong>In-hospital mortality did not differ by VTE timing or anticoagulation status. However, hemorrhage expansion was more frequent in early VTE patients, particularly those with subdural hematomas, emphasizing the need for individualized anticoagulation strategies.</p>\",\"PeriodicalId\":94220,\"journal\":{\"name\":\"TH open : companion journal to thrombosis and haemostasis\",\"volume\":\"9 \",\"pages\":\"a26161673\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12223956/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"TH open : companion journal to thrombosis and haemostasis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2616-1673\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2616-1673","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
In-Hospital Mortality and Hemorrhagic Risks in Traumatic Brain Injury Patients with Early vs. Late Venous Thromboembolism.
Objective: This study reviewed the management and outcomes of traumatic brain injury (TBI) patients who developed venous thromboembolism (VTE) during hospitalization, focusing on the timing of VTE diagnosis and anticoagulation initiation.
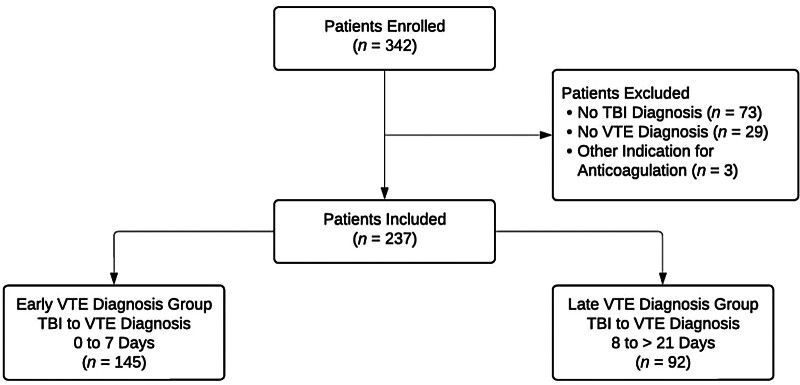
Methods: This retrospective, single-center study utilized data from the University of Texas Trauma Database. Patients were categorized based on VTE diagnosis timing (early ≤7 days, late >7 days). The primary outcome was in-hospital mortality. Secondary outcomes included mortality specifically among patients who were receiving anticoagulation treatment, hemorrhagic complications, predictors associated with early anticoagulation initiation (defined as ≤ 7 days from VTE diagnosis), and whether anticoagulation timing influenced mortality.
Results: Among 237 patients (early: 145, late: 92), the mean age was 59 ± 20 years vs. 55 ± 20 years ( p = 0.133). Males comprised 68% vs. 78% ( p = 0.038). Subdural hematomas were the predominant injury (63% vs. 68%, p = 0.443). In-hospital mortality was similar (10% vs. 13%, p = 0.524) and did not differ between anticoagulated and non-anticoagulated patients ( p = 0.94). Among patients who died, 73% in the early group and 100% in the late group had received anticoagulation ( p = 0.053). Hemorrhage expansion was more frequent in early VTE patients (40% vs. 0%, p = 0.046). Pulmonary embolism was associated with early anticoagulation (OR = 1.86, 95% CI: 1.09-3.17, p = 0.023), while severe neurologic injury (GCS <9) reduced its likelihood (OR = 0.53, 95% CI: 0.28-0.98, p = 0.042).
Conclusion: In-hospital mortality did not differ by VTE timing or anticoagulation status. However, hemorrhage expansion was more frequent in early VTE patients, particularly those with subdural hematomas, emphasizing the need for individualized anticoagulation strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


