Heleen van Aswegen, Ronel Roos, Elizma Haarhoff, Josslyn de Kock, Humairaa Ebrahim, Sameer Tootla, Muhammad Vally, Monika Fagevik Olsén
{"title":"中低社会经济地位胸椎创伤患者的概况及处理。","authors":"Heleen van Aswegen, Ronel Roos, Elizma Haarhoff, Josslyn de Kock, Humairaa Ebrahim, Sameer Tootla, Muhammad Vally, Monika Fagevik Olsén","doi":"10.4102/sajp.v81i1.2146","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pain and shortness of breath (SOB) after thoracic trauma predispose patients to complications and prolonged hospital length of stay (LOS). Patient management after thoracic trauma is seldom reported.</p><p><strong>Objectives: </strong>To describe patient profiles, symptoms, management, adverse events, complications, discharge destinations and follow-up referral services.</p><p><strong>Method: </strong>Prospective observational design using clinical record review at two university-affiliated hospitals over 18 months. Adults with thoracic trauma diagnosis were consecutively screened for inclusion. Study objectives guided information retrieved from records. Statistical analyses were done with significance at <i>p</i>< 0.05.</p><p><strong>Results: </strong>Most were male (<i>n</i> = 170/179; 95%). Penetrating trauma following assault was common (<i>n</i> = 146/179; 82%). Conservative management included analgesia (<i>n</i> = 176/178; 98%) and intercostal drain insertion (<i>n</i> = 165/179; 92%). Physiotherapists treated patients daily. Management involved functional activities (cycling [<i>n</i> = 71/149; 48%], early mobilisation [<i>n</i> = 120/174; 69%]), lung volume enhancement (deep breathing exercises [<i>n</i> = 97/174; 56%], positive expiratory pressure [<i>n</i> = 98/174; 56%]), secretion removal (active coughing [<i>n</i> = 60/174; 34%]). Shoulder (<i>n</i> = 43/174; 25%) and trunk (<i>n</i> = 6/153; 4%) ROM were seldom done. Blunt trauma caused higher pain during deep breathing (median 7/10; IQR: 3.5-8.0) versus penetrating trauma (median 4/10; IQR: 2.0-7.5; <i>p</i>= 0.04). Most reported 'slight' to 'very slight' SOB. Time out-of-bed and distance walked increased daily with smokers mobilising away from bed frequently (<i>n</i> = 73/95; 77%). Few adverse events and complications occurred. Mean LOS was 5.5 ± 4.3 days. Most were discharged home (<i>n</i> = 177/179; 99%); two were referred for follow-up physiotherapy.</p><p><strong>Conclusion: </strong>Management is guided by individual patient needs. Treatment comprises early mobilisation, lung volume enhancement, and secretion removal with less attention on ROM exercises and post-discharge services.</p><p><strong>Clinical implications: </strong>Shoulder and trunk ROM should be prioritised. Service delivery approaches need review considering the evidence.</p>","PeriodicalId":44180,"journal":{"name":"South African Journal of Physiotherapy","volume":"81 1","pages":"2146"},"PeriodicalIF":1.2000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12224066/pdf/","citationCount":"0","resultStr":"{\"title\":\"Profile and management of patients from low-middle socioeconomic status with thoracic trauma.\",\"authors\":\"Heleen van Aswegen, Ronel Roos, Elizma Haarhoff, Josslyn de Kock, Humairaa Ebrahim, Sameer Tootla, Muhammad Vally, Monika Fagevik Olsén\",\"doi\":\"10.4102/sajp.v81i1.2146\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pain and shortness of breath (SOB) after thoracic trauma predispose patients to complications and prolonged hospital length of stay (LOS). Patient management after thoracic trauma is seldom reported.</p><p><strong>Objectives: </strong>To describe patient profiles, symptoms, management, adverse events, complications, discharge destinations and follow-up referral services.</p><p><strong>Method: </strong>Prospective observational design using clinical record review at two university-affiliated hospitals over 18 months. Adults with thoracic trauma diagnosis were consecutively screened for inclusion. Study objectives guided information retrieved from records. Statistical analyses were done with significance at <i>p</i>< 0.05.</p><p><strong>Results: </strong>Most were male (<i>n</i> = 170/179; 95%). Penetrating trauma following assault was common (<i>n</i> = 146/179; 82%). Conservative management included analgesia (<i>n</i> = 176/178; 98%) and intercostal drain insertion (<i>n</i> = 165/179; 92%). Physiotherapists treated patients daily. Management involved functional activities (cycling [<i>n</i> = 71/149; 48%], early mobilisation [<i>n</i> = 120/174; 69%]), lung volume enhancement (deep breathing exercises [<i>n</i> = 97/174; 56%], positive expiratory pressure [<i>n</i> = 98/174; 56%]), secretion removal (active coughing [<i>n</i> = 60/174; 34%]). Shoulder (<i>n</i> = 43/174; 25%) and trunk (<i>n</i> = 6/153; 4%) ROM were seldom done. Blunt trauma caused higher pain during deep breathing (median 7/10; IQR: 3.5-8.0) versus penetrating trauma (median 4/10; IQR: 2.0-7.5; <i>p</i>= 0.04). Most reported 'slight' to 'very slight' SOB. Time out-of-bed and distance walked increased daily with smokers mobilising away from bed frequently (<i>n</i> = 73/95; 77%). Few adverse events and complications occurred. Mean LOS was 5.5 ± 4.3 days. Most were discharged home (<i>n</i> = 177/179; 99%); two were referred for follow-up physiotherapy.</p><p><strong>Conclusion: </strong>Management is guided by individual patient needs. Treatment comprises early mobilisation, lung volume enhancement, and secretion removal with less attention on ROM exercises and post-discharge services.</p><p><strong>Clinical implications: </strong>Shoulder and trunk ROM should be prioritised. Service delivery approaches need review considering the evidence.</p>\",\"PeriodicalId\":44180,\"journal\":{\"name\":\"South African Journal of Physiotherapy\",\"volume\":\"81 1\",\"pages\":\"2146\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12224066/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"South African Journal of Physiotherapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/sajp.v81i1.2146\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"REHABILITATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"South African Journal of Physiotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/sajp.v81i1.2146","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"REHABILITATION","Score":null,"Total":0}
Profile and management of patients from low-middle socioeconomic status with thoracic trauma.
Background: Pain and shortness of breath (SOB) after thoracic trauma predispose patients to complications and prolonged hospital length of stay (LOS). Patient management after thoracic trauma is seldom reported.
Objectives: To describe patient profiles, symptoms, management, adverse events, complications, discharge destinations and follow-up referral services.
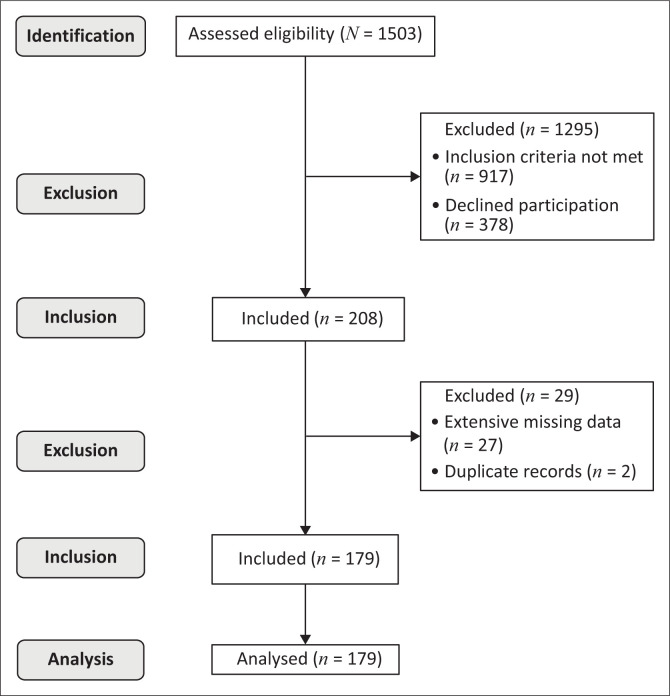
Method: Prospective observational design using clinical record review at two university-affiliated hospitals over 18 months. Adults with thoracic trauma diagnosis were consecutively screened for inclusion. Study objectives guided information retrieved from records. Statistical analyses were done with significance at p< 0.05.
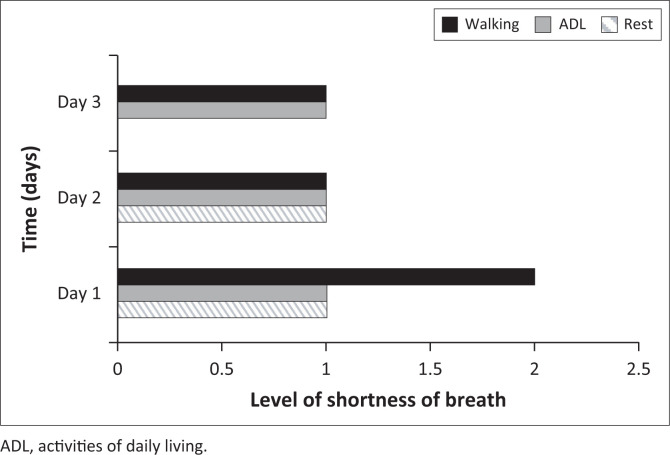
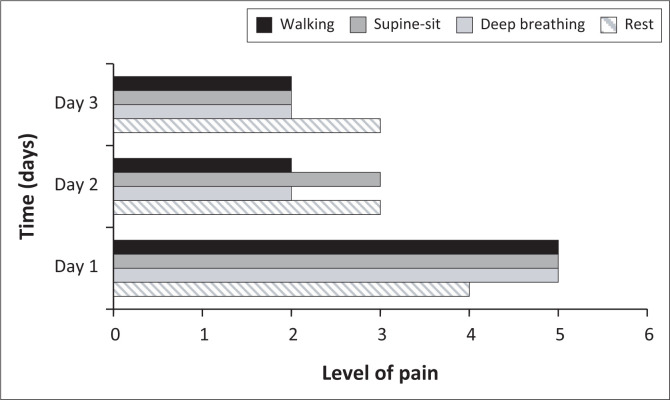
Results: Most were male (n = 170/179; 95%). Penetrating trauma following assault was common (n = 146/179; 82%). Conservative management included analgesia (n = 176/178; 98%) and intercostal drain insertion (n = 165/179; 92%). Physiotherapists treated patients daily. Management involved functional activities (cycling [n = 71/149; 48%], early mobilisation [n = 120/174; 69%]), lung volume enhancement (deep breathing exercises [n = 97/174; 56%], positive expiratory pressure [n = 98/174; 56%]), secretion removal (active coughing [n = 60/174; 34%]). Shoulder (n = 43/174; 25%) and trunk (n = 6/153; 4%) ROM were seldom done. Blunt trauma caused higher pain during deep breathing (median 7/10; IQR: 3.5-8.0) versus penetrating trauma (median 4/10; IQR: 2.0-7.5; p= 0.04). Most reported 'slight' to 'very slight' SOB. Time out-of-bed and distance walked increased daily with smokers mobilising away from bed frequently (n = 73/95; 77%). Few adverse events and complications occurred. Mean LOS was 5.5 ± 4.3 days. Most were discharged home (n = 177/179; 99%); two were referred for follow-up physiotherapy.
Conclusion: Management is guided by individual patient needs. Treatment comprises early mobilisation, lung volume enhancement, and secretion removal with less attention on ROM exercises and post-discharge services.
Clinical implications: Shoulder and trunk ROM should be prioritised. Service delivery approaches need review considering the evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


