Nicolas Polge, Camille Hego, Jules Grégory, Sophie Hamada, Anne Godier, Jean Charles Bijot, Axelle Dupont, Paer-Selim Abback, Caroline Jeantrelle, Emmanuel Weiss, Jean Denis Moyer
{"title":"重症监护室严重脾外伤及其处理对感染发生的影响。","authors":"Nicolas Polge, Camille Hego, Jules Grégory, Sophie Hamada, Anne Godier, Jean Charles Bijot, Axelle Dupont, Paer-Selim Abback, Caroline Jeantrelle, Emmanuel Weiss, Jean Denis Moyer","doi":"10.1136/tsaco-2024-001704","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Severe trauma can be responsible for a major systemic inflammatory response followed by post-traumatic immunosuppression. Immune imbalance promotes infections and increases mortality. This risk could be further increased in case of impaired splenic immune function due to splenic trauma. The objective of this study was to evaluate whether severe splenic trauma increased infectious complications in trauma patients during intensive care unit (ICU) stay.</p><p><strong>Methods: </strong>This was an observational, bicentric, retrospective, case-control study including patients admitted for severe trauma from January 2011 to December 2020 in two level 1 trauma centers. Patients with American Association for the Surgery of Trauma (AAST) ≥III splenic trauma (case) were matched (1:3) with patients without splenic trauma (controls) according to age, sex, Injury Severity Score, initial Glasgow Coma Score, and Simplified Acute Physiology Score II. Demographic, trauma management, and infection data were collected. The primary endpoint was the incidence density of any infectious disease during ICU stay.</p><p><strong>Results: </strong>Among 7,304 severe trauma patients, 130 patients with AAST ≥III splenic trauma were included. 10 patients could not be matched with controls. 17 patients (14.1%) underwent splenectomy, 56 patients (46.7%) had non-operative management with arterioembolization, and 47 (39.2%) had non-operative management without embolization. There was no difference between cases and controls regarding incidence density of infections (44.1 (34.6-55.5)/1,000 person days vs 43.6 (37.7-50.2)/1,000 person days, incidence rate ratio=1 95% CI (0.77 to 1.3) p=0.94), type of infection, involved microorganisms, or severity (septic shock 12% vs 9.2%, p=0.6; acute respiratory distress syndrome 14% vs 9.2%, p=0.2).</p><p><strong>Conclusion: </strong>In the present study, AAST ≥III splenic trauma in severe trauma patients was not associated with an increased risk of infection during ICU stay.Level of evidence III.</p>","PeriodicalId":23307,"journal":{"name":"Trauma Surgery & Acute Care Open","volume":"10 3","pages":"e001704"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215103/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of severe splenic trauma and its management on the occurrence of infections in intensive care unit.\",\"authors\":\"Nicolas Polge, Camille Hego, Jules Grégory, Sophie Hamada, Anne Godier, Jean Charles Bijot, Axelle Dupont, Paer-Selim Abback, Caroline Jeantrelle, Emmanuel Weiss, Jean Denis Moyer\",\"doi\":\"10.1136/tsaco-2024-001704\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Severe trauma can be responsible for a major systemic inflammatory response followed by post-traumatic immunosuppression. Immune imbalance promotes infections and increases mortality. This risk could be further increased in case of impaired splenic immune function due to splenic trauma. The objective of this study was to evaluate whether severe splenic trauma increased infectious complications in trauma patients during intensive care unit (ICU) stay.</p><p><strong>Methods: </strong>This was an observational, bicentric, retrospective, case-control study including patients admitted for severe trauma from January 2011 to December 2020 in two level 1 trauma centers. Patients with American Association for the Surgery of Trauma (AAST) ≥III splenic trauma (case) were matched (1:3) with patients without splenic trauma (controls) according to age, sex, Injury Severity Score, initial Glasgow Coma Score, and Simplified Acute Physiology Score II. Demographic, trauma management, and infection data were collected. The primary endpoint was the incidence density of any infectious disease during ICU stay.</p><p><strong>Results: </strong>Among 7,304 severe trauma patients, 130 patients with AAST ≥III splenic trauma were included. 10 patients could not be matched with controls. 17 patients (14.1%) underwent splenectomy, 56 patients (46.7%) had non-operative management with arterioembolization, and 47 (39.2%) had non-operative management without embolization. There was no difference between cases and controls regarding incidence density of infections (44.1 (34.6-55.5)/1,000 person days vs 43.6 (37.7-50.2)/1,000 person days, incidence rate ratio=1 95% CI (0.77 to 1.3) p=0.94), type of infection, involved microorganisms, or severity (septic shock 12% vs 9.2%, p=0.6; acute respiratory distress syndrome 14% vs 9.2%, p=0.2).</p><p><strong>Conclusion: </strong>In the present study, AAST ≥III splenic trauma in severe trauma patients was not associated with an increased risk of infection during ICU stay.Level of evidence III.</p>\",\"PeriodicalId\":23307,\"journal\":{\"name\":\"Trauma Surgery & Acute Care Open\",\"volume\":\"10 3\",\"pages\":\"e001704\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215103/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Trauma Surgery & Acute Care Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/tsaco-2024-001704\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Trauma Surgery & Acute Care Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/tsaco-2024-001704","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的:严重创伤可导致主要的全身炎症反应,随后是创伤后免疫抑制。免疫失衡促进感染,增加死亡率。如果脾外伤导致脾免疫功能受损,这种风险可能进一步增加。本研究的目的是评估严重脾损伤是否会增加重症监护病房(ICU)创伤患者的感染并发症。方法:这是一项观察性、双中心、回顾性、病例对照研究,纳入了2011年1月至2020年12月在两个一级创伤中心收治的严重创伤患者。根据年龄、性别、损伤严重程度评分、初始格拉斯哥昏迷评分和简化急性生理评分II,将美国创伤外科协会(AAST)≥III型脾损伤患者(病例)与无脾损伤患者(对照组)按1:3匹配。收集人口统计、创伤管理和感染数据。主要终点是ICU住院期间任何传染病的发病率密度。结果:7304例重型创伤患者中,AAST≥III级脾损伤患者共纳入130例。10例患者不能与对照组匹配。脾切除术17例(14.1%),非手术加动脉栓塞56例(46.7%),非手术加动脉栓塞47例(39.2%)。病例和对照组在感染发生率密度(44.1(34.6-55.5)/ 1000人天vs 43.6(37.7-50.2)/ 1000人天,发病率比=1 95% CI (0.77 - 1.3) p=0.94)、感染类型、涉及的微生物或严重程度(感染性休克12% vs 9.2%, p=0.6;急性呼吸窘迫综合征(14% vs 9.2%, p=0.2)。结论:在本研究中,严重创伤患者AAST≥III级脾损伤与ICU住院期间感染风险增加无关。证据水平III。
Impact of severe splenic trauma and its management on the occurrence of infections in intensive care unit.
Purpose: Severe trauma can be responsible for a major systemic inflammatory response followed by post-traumatic immunosuppression. Immune imbalance promotes infections and increases mortality. This risk could be further increased in case of impaired splenic immune function due to splenic trauma. The objective of this study was to evaluate whether severe splenic trauma increased infectious complications in trauma patients during intensive care unit (ICU) stay.
Methods: This was an observational, bicentric, retrospective, case-control study including patients admitted for severe trauma from January 2011 to December 2020 in two level 1 trauma centers. Patients with American Association for the Surgery of Trauma (AAST) ≥III splenic trauma (case) were matched (1:3) with patients without splenic trauma (controls) according to age, sex, Injury Severity Score, initial Glasgow Coma Score, and Simplified Acute Physiology Score II. Demographic, trauma management, and infection data were collected. The primary endpoint was the incidence density of any infectious disease during ICU stay.
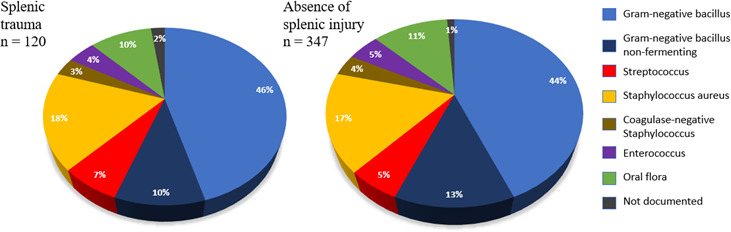
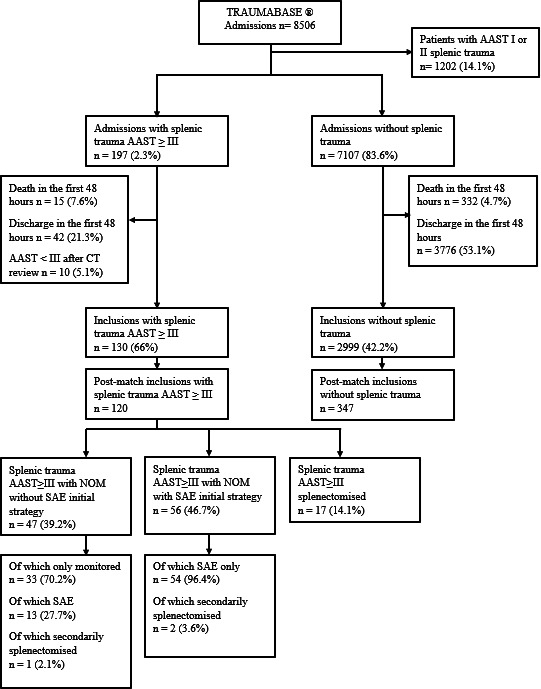
Results: Among 7,304 severe trauma patients, 130 patients with AAST ≥III splenic trauma were included. 10 patients could not be matched with controls. 17 patients (14.1%) underwent splenectomy, 56 patients (46.7%) had non-operative management with arterioembolization, and 47 (39.2%) had non-operative management without embolization. There was no difference between cases and controls regarding incidence density of infections (44.1 (34.6-55.5)/1,000 person days vs 43.6 (37.7-50.2)/1,000 person days, incidence rate ratio=1 95% CI (0.77 to 1.3) p=0.94), type of infection, involved microorganisms, or severity (septic shock 12% vs 9.2%, p=0.6; acute respiratory distress syndrome 14% vs 9.2%, p=0.2).
Conclusion: In the present study, AAST ≥III splenic trauma in severe trauma patients was not associated with an increased risk of infection during ICU stay.Level of evidence III.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


