Kate Sugar, Candy McCabe, Alison Llewellyn, Wayne de Leeuw, Maggie Crowe, Claire Prendergast, Charlotte Spence, Natasha Bradley
{"title":"安宁疗护社区服务重新设计之实施:确定经验教训之定性研究。","authors":"Kate Sugar, Candy McCabe, Alison Llewellyn, Wayne de Leeuw, Maggie Crowe, Claire Prendergast, Charlotte Spence, Natasha Bradley","doi":"10.1177/26323524251349839","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The need to improve equity of access to palliative care is well recognized; however, much less is known about how new models of hospice community services can be successfully introduced.</p><p><strong>Aim: </strong>We aimed to capture learning from the implementation experiences of hospice stakeholders during the first 12 months of a hospice community services redesign.</p><p><strong>Design: </strong>Qualitative research using individual semi-structured interviews (<i>n</i> = 38) and follow-up focus groups (<i>n</i> = 8).</p><p><strong>Methods: </strong>Participants were clinical and non-clinical staff, hospice leaders, volunteers, and external stakeholders. Interviews were analysed with framework analysis using Normalisation Process Theory. Focus groups were used to confirm and prioritise recommendations.</p><p><strong>Results: </strong>Implementation is more likely to be successful where hospice personnel are enabled to work together in understanding and adapting to new ways of working. Participants gave examples of being supported to plan activities, to form networks of participation, to pilot new ways of working, and to appraise and improve their work. Receiving feedback on progress is beneficial. Implementation strategies that are tailored to each context could be effective if they engage with hospice stakeholders to ensure that strategic aims are well-understood and that the necessary resources are available. Positive experiences of implementation are more likely where stakeholders understand the changes and can participate in planning. Where necessary, changes to human resources and technology support systems would ideally be adopted prior to making changes to patient-facing services.</p><p><strong>Conclusion: </strong>This study contributes knowledge from a charitable provider of specialist palliative care during the implementation of a hospice community service redesign. We identified opportunities for future improvement, particularly regarding communication, planning, prioritisation, and feedback. Investment of time and reflection during implementation can support the ambition of hospices to become integrated within a place-based system, to improve access to palliative care within the communities they serve. We report key implementation recommendations for organisations considering service redesign.</p>","PeriodicalId":36693,"journal":{"name":"Palliative Care and Social Practice","volume":"19 ","pages":"26323524251349839"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214322/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation of a hospice community service redesign: Qualitative research identifying lessons learned.\",\"authors\":\"Kate Sugar, Candy McCabe, Alison Llewellyn, Wayne de Leeuw, Maggie Crowe, Claire Prendergast, Charlotte Spence, Natasha Bradley\",\"doi\":\"10.1177/26323524251349839\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The need to improve equity of access to palliative care is well recognized; however, much less is known about how new models of hospice community services can be successfully introduced.</p><p><strong>Aim: </strong>We aimed to capture learning from the implementation experiences of hospice stakeholders during the first 12 months of a hospice community services redesign.</p><p><strong>Design: </strong>Qualitative research using individual semi-structured interviews (<i>n</i> = 38) and follow-up focus groups (<i>n</i> = 8).</p><p><strong>Methods: </strong>Participants were clinical and non-clinical staff, hospice leaders, volunteers, and external stakeholders. Interviews were analysed with framework analysis using Normalisation Process Theory. Focus groups were used to confirm and prioritise recommendations.</p><p><strong>Results: </strong>Implementation is more likely to be successful where hospice personnel are enabled to work together in understanding and adapting to new ways of working. Participants gave examples of being supported to plan activities, to form networks of participation, to pilot new ways of working, and to appraise and improve their work. Receiving feedback on progress is beneficial. Implementation strategies that are tailored to each context could be effective if they engage with hospice stakeholders to ensure that strategic aims are well-understood and that the necessary resources are available. Positive experiences of implementation are more likely where stakeholders understand the changes and can participate in planning. Where necessary, changes to human resources and technology support systems would ideally be adopted prior to making changes to patient-facing services.</p><p><strong>Conclusion: </strong>This study contributes knowledge from a charitable provider of specialist palliative care during the implementation of a hospice community service redesign. We identified opportunities for future improvement, particularly regarding communication, planning, prioritisation, and feedback. Investment of time and reflection during implementation can support the ambition of hospices to become integrated within a place-based system, to improve access to palliative care within the communities they serve. We report key implementation recommendations for organisations considering service redesign.</p>\",\"PeriodicalId\":36693,\"journal\":{\"name\":\"Palliative Care and Social Practice\",\"volume\":\"19 \",\"pages\":\"26323524251349839\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214322/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Palliative Care and Social Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26323524251349839\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care and Social Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26323524251349839","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Implementation of a hospice community service redesign: Qualitative research identifying lessons learned.
Background: The need to improve equity of access to palliative care is well recognized; however, much less is known about how new models of hospice community services can be successfully introduced.
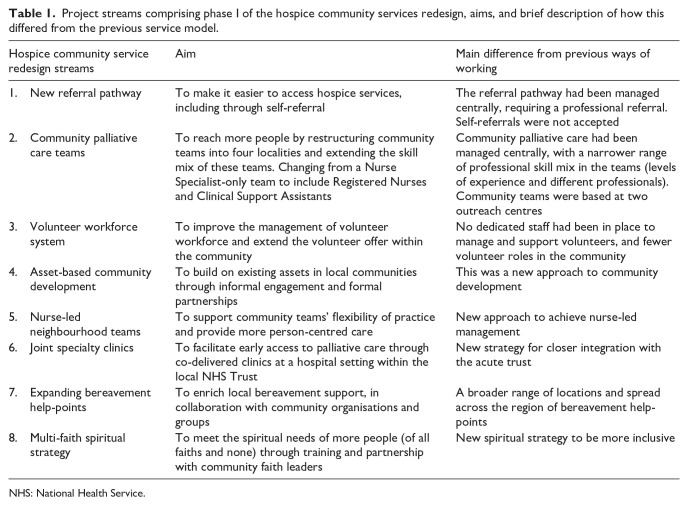
Aim: We aimed to capture learning from the implementation experiences of hospice stakeholders during the first 12 months of a hospice community services redesign.
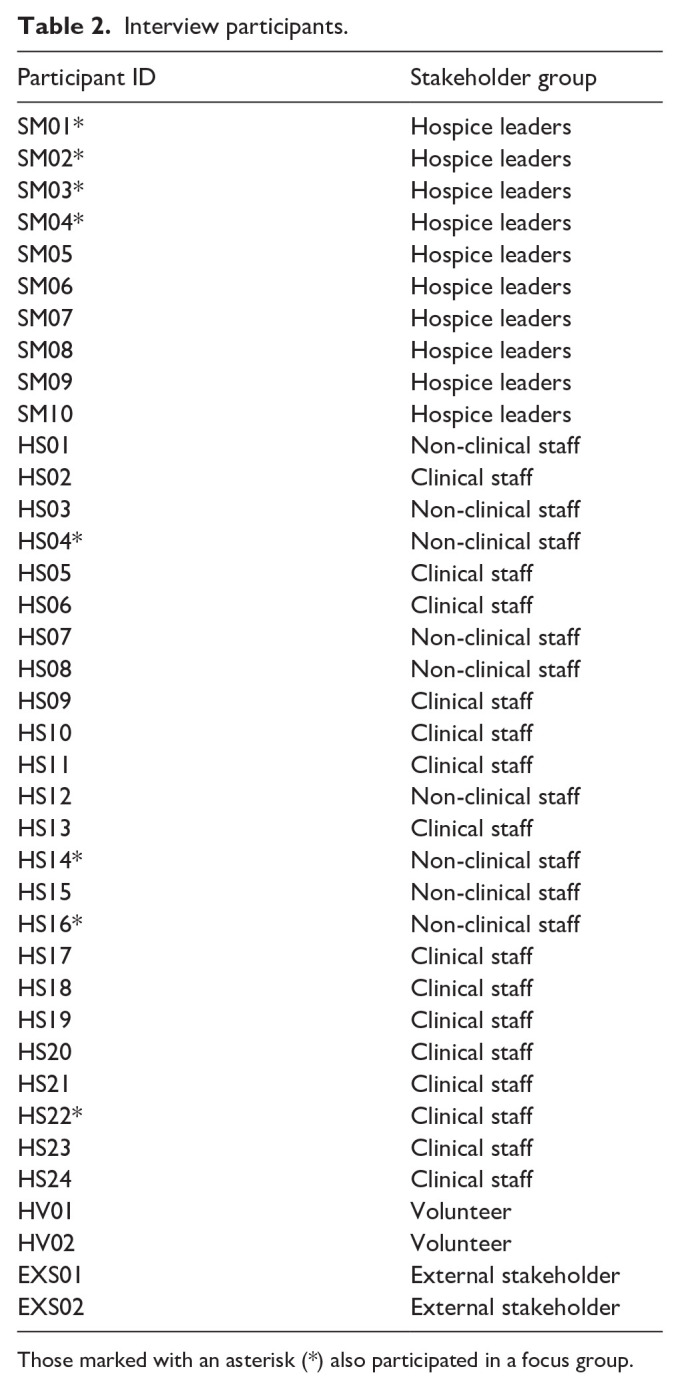
Design: Qualitative research using individual semi-structured interviews (n = 38) and follow-up focus groups (n = 8).
Methods: Participants were clinical and non-clinical staff, hospice leaders, volunteers, and external stakeholders. Interviews were analysed with framework analysis using Normalisation Process Theory. Focus groups were used to confirm and prioritise recommendations.
Results: Implementation is more likely to be successful where hospice personnel are enabled to work together in understanding and adapting to new ways of working. Participants gave examples of being supported to plan activities, to form networks of participation, to pilot new ways of working, and to appraise and improve their work. Receiving feedback on progress is beneficial. Implementation strategies that are tailored to each context could be effective if they engage with hospice stakeholders to ensure that strategic aims are well-understood and that the necessary resources are available. Positive experiences of implementation are more likely where stakeholders understand the changes and can participate in planning. Where necessary, changes to human resources and technology support systems would ideally be adopted prior to making changes to patient-facing services.
Conclusion: This study contributes knowledge from a charitable provider of specialist palliative care during the implementation of a hospice community service redesign. We identified opportunities for future improvement, particularly regarding communication, planning, prioritisation, and feedback. Investment of time and reflection during implementation can support the ambition of hospices to become integrated within a place-based system, to improve access to palliative care within the communities they serve. We report key implementation recommendations for organisations considering service redesign.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


