{"title":"急性心肌梗死相关性心源性休克中静脉-动脉体外膜氧合的预后意义。","authors":"Jonghu Shin, Eun-Mi Kang, Sang-Hyup Lee, Minju Heo, Yong-Joon Lee, Seung-Jun Lee, Sung-Jin Hong, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Donghoon Choi, Myeong-Ki Hong, Yangsoo Jang, Chul-Min Ahn","doi":"10.1186/s40560-025-00807-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Given the conflicting results regarding the clinical outcomes of venoarterial extracorporeal membrane oxygenation (VA-ECMO) based on etiology, its benefit for patients with cardiogenic shock (CS) remains controversial. This study aimed to report the real-world clinical outcomes of VA-ECMO treatment for patients with CS, based on the presence of acute myocardial infarction (AMI).</p><p><strong>Methods: </strong>Patients treated with peripheral VA-ECMO between 2008 and 2023 at a tertiary cardiovascular center were included and classified into two groups based on CS etiology (AMI-CS and non-AMI-CS). Logistic regression models were used to compare in-hospital mortality and to identify prognostic predictors.</p><p><strong>Results: </strong>Among the 667 patients included, 264 (39.6%) were classified as having AMI-CS. The rate of cardiac arrest before VA-ECMO initiation was higher in the AMI-CS group than in the non-AMI-CS group (69.7% vs. 55.8%; P < 0.001). Patients in the AMI-CS group were older (66 vs. 61 years; P < 0.001), more likely to be male (82.6% vs. 57.3%; P < 0.001), and had a lower left ventricular (LV) ejection fraction (20% vs. 25%; P < 0.001) than those in the non-AMI-CS group. The AMI-CS group had a lower in-hospital mortality rate (58.6% vs. 69.7%; odds ratio, 0.46; 95% confidence interval, 0.29-0.75; P = 0.002) compared with the non-AMI-CS group. The independent predictors of favorable clinical outcomes after VA-ECMO included younger age, shorter cardiac arrest duration, absence of severe LV dysfunction, absence of renal replacement therapy, higher hemoglobin levels, higher arterial pH, and lower lactate levels. The association between in-hospital mortality and AMI-CS was also demonstrated in the propensity score matching analysis.</p><p><strong>Conclusions: </strong>In this single-center study, AMI-CS was associated with a lower in-hospital mortality than non-AMI-CS after VA-ECMO treatment.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"38"},"PeriodicalIF":4.7000,"publicationDate":"2025-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12219146/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic implication of venoarterial extracorporeal membrane oxygenation in acute myocardial infarction-related cardiogenic shock.\",\"authors\":\"Jonghu Shin, Eun-Mi Kang, Sang-Hyup Lee, Minju Heo, Yong-Joon Lee, Seung-Jun Lee, Sung-Jin Hong, Jung-Sun Kim, Byeong-Keuk Kim, Young-Guk Ko, Donghoon Choi, Myeong-Ki Hong, Yangsoo Jang, Chul-Min Ahn\",\"doi\":\"10.1186/s40560-025-00807-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Given the conflicting results regarding the clinical outcomes of venoarterial extracorporeal membrane oxygenation (VA-ECMO) based on etiology, its benefit for patients with cardiogenic shock (CS) remains controversial. This study aimed to report the real-world clinical outcomes of VA-ECMO treatment for patients with CS, based on the presence of acute myocardial infarction (AMI).</p><p><strong>Methods: </strong>Patients treated with peripheral VA-ECMO between 2008 and 2023 at a tertiary cardiovascular center were included and classified into two groups based on CS etiology (AMI-CS and non-AMI-CS). Logistic regression models were used to compare in-hospital mortality and to identify prognostic predictors.</p><p><strong>Results: </strong>Among the 667 patients included, 264 (39.6%) were classified as having AMI-CS. The rate of cardiac arrest before VA-ECMO initiation was higher in the AMI-CS group than in the non-AMI-CS group (69.7% vs. 55.8%; P < 0.001). Patients in the AMI-CS group were older (66 vs. 61 years; P < 0.001), more likely to be male (82.6% vs. 57.3%; P < 0.001), and had a lower left ventricular (LV) ejection fraction (20% vs. 25%; P < 0.001) than those in the non-AMI-CS group. The AMI-CS group had a lower in-hospital mortality rate (58.6% vs. 69.7%; odds ratio, 0.46; 95% confidence interval, 0.29-0.75; P = 0.002) compared with the non-AMI-CS group. The independent predictors of favorable clinical outcomes after VA-ECMO included younger age, shorter cardiac arrest duration, absence of severe LV dysfunction, absence of renal replacement therapy, higher hemoglobin levels, higher arterial pH, and lower lactate levels. The association between in-hospital mortality and AMI-CS was also demonstrated in the propensity score matching analysis.</p><p><strong>Conclusions: </strong>In this single-center study, AMI-CS was associated with a lower in-hospital mortality than non-AMI-CS after VA-ECMO treatment.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"13 1\",\"pages\":\"38\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2025-07-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12219146/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-025-00807-w\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00807-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
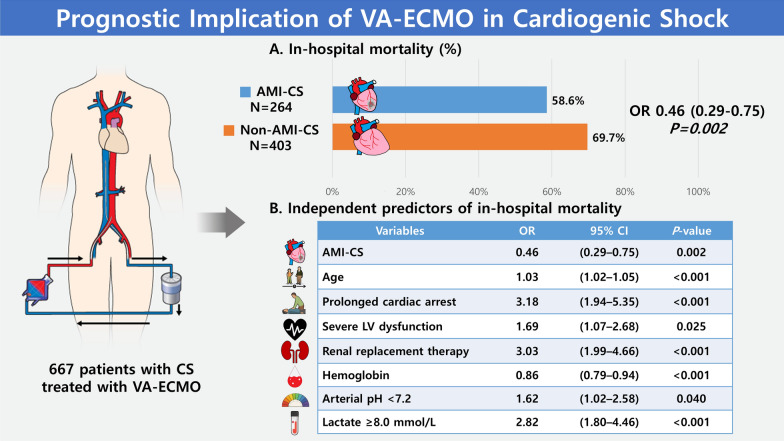
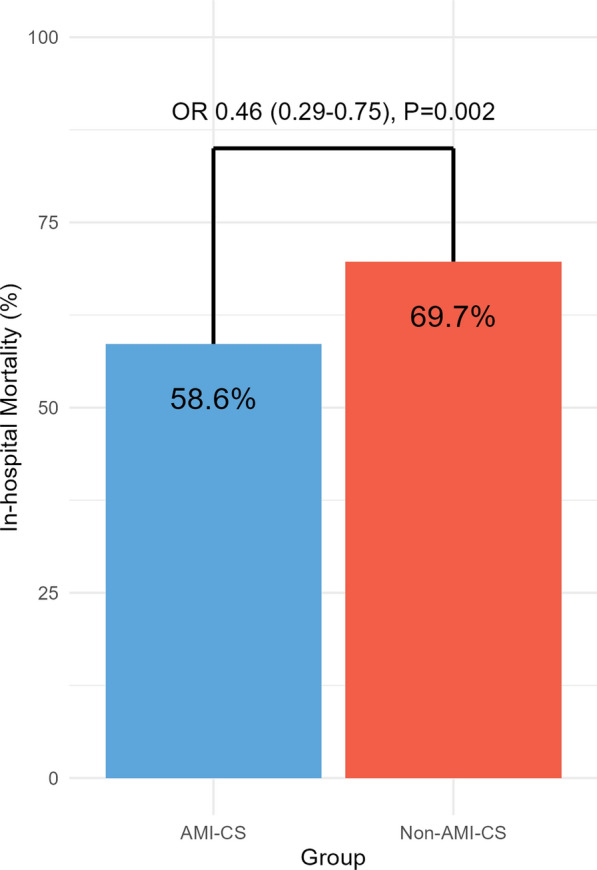
背景:鉴于基于病因的静脉动脉体外膜氧合(VA-ECMO)的临床结果相互矛盾,其对心源性休克(CS)患者的益处仍存在争议。本研究旨在报道基于急性心肌梗死(AMI)存在的CS患者VA-ECMO治疗的真实临床结果。方法:纳入2008 - 2023年在三级心血管中心接受外周VA-ECMO治疗的患者,并根据CS病因分为AMI-CS和非AMI-CS两组。使用逻辑回归模型比较住院死亡率并确定预后预测因子。结果:667例患者中,264例(39.6%)为AMI-CS。AMI-CS组在VA-ECMO开始前的心脏骤停率高于非AMI-CS组(69.7% vs. 55.8%;结论:在这项单中心研究中,AMI-CS在VA-ECMO治疗后的住院死亡率低于非AMI-CS。
Prognostic implication of venoarterial extracorporeal membrane oxygenation in acute myocardial infarction-related cardiogenic shock.
Background: Given the conflicting results regarding the clinical outcomes of venoarterial extracorporeal membrane oxygenation (VA-ECMO) based on etiology, its benefit for patients with cardiogenic shock (CS) remains controversial. This study aimed to report the real-world clinical outcomes of VA-ECMO treatment for patients with CS, based on the presence of acute myocardial infarction (AMI).
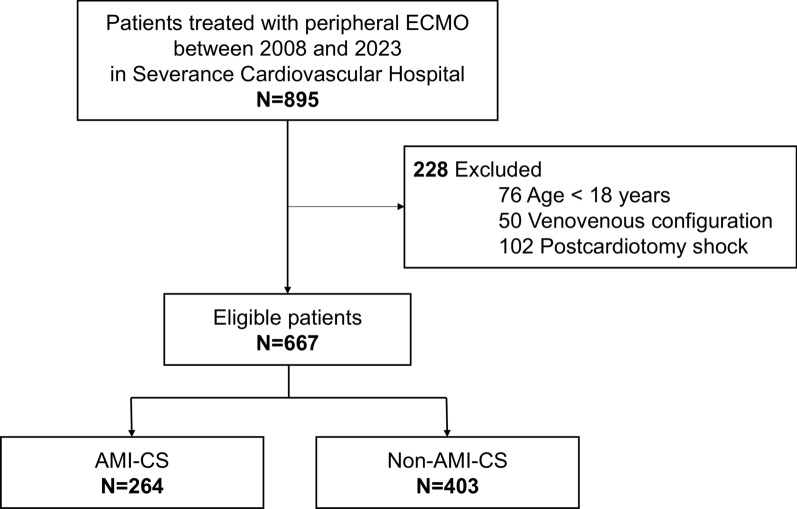
Methods: Patients treated with peripheral VA-ECMO between 2008 and 2023 at a tertiary cardiovascular center were included and classified into two groups based on CS etiology (AMI-CS and non-AMI-CS). Logistic regression models were used to compare in-hospital mortality and to identify prognostic predictors.
Results: Among the 667 patients included, 264 (39.6%) were classified as having AMI-CS. The rate of cardiac arrest before VA-ECMO initiation was higher in the AMI-CS group than in the non-AMI-CS group (69.7% vs. 55.8%; P < 0.001). Patients in the AMI-CS group were older (66 vs. 61 years; P < 0.001), more likely to be male (82.6% vs. 57.3%; P < 0.001), and had a lower left ventricular (LV) ejection fraction (20% vs. 25%; P < 0.001) than those in the non-AMI-CS group. The AMI-CS group had a lower in-hospital mortality rate (58.6% vs. 69.7%; odds ratio, 0.46; 95% confidence interval, 0.29-0.75; P = 0.002) compared with the non-AMI-CS group. The independent predictors of favorable clinical outcomes after VA-ECMO included younger age, shorter cardiac arrest duration, absence of severe LV dysfunction, absence of renal replacement therapy, higher hemoglobin levels, higher arterial pH, and lower lactate levels. The association between in-hospital mortality and AMI-CS was also demonstrated in the propensity score matching analysis.
Conclusions: In this single-center study, AMI-CS was associated with a lower in-hospital mortality than non-AMI-CS after VA-ECMO treatment.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


