Rubén Alonso-Beato, Pablo Demelo-Rodríguez, Lucía Ordieres-Ortega, Marina López-Rubio, Marta-Olimpia Lago-Rodríguez, Crhistian-Mario Oblitas, Luis Antonio Alvarez-Sala Walther, Francisco Galeano-Valle
{"title":"covid -19相关静脉血栓栓塞的短期和长期结局:一项倾向评分匹配的队列研究","authors":"Rubén Alonso-Beato, Pablo Demelo-Rodríguez, Lucía Ordieres-Ortega, Marina López-Rubio, Marta-Olimpia Lago-Rodríguez, Crhistian-Mario Oblitas, Luis Antonio Alvarez-Sala Walther, Francisco Galeano-Valle","doi":"10.1007/s11739-025-04042-x","DOIUrl":null,"url":null,"abstract":"<p><p>Venous thromboembolism (VTE) is a recognized complication of SARS-CoV-2 infection, but its clinical features and both sort- and long-term outcomes remain incompletely characterized. We aimed to compare the clinical profile and outcomes of patients with VTE with and without recent COVID-19. We conducted a prospective cohort study including 2012 patients with objectively confirmed VTE. COVID-19-associated VTE was defined as VTE diagnosed within 30 days of a microbiologically confirmed SARS-CoV-2 infection. Clinical characteristics, treatment, and outcomes were compared between groups. Propensity score matching (1:1) and competing risk models were used to adjust for confounding. The primary outcomes-assessed at both 30 days and 365 days-included all-cause mortality, major bleeding, and VTE recurrence. A total of 272 patients (13.5%) had COVID-19-associated VTE. Compared with non-COVID cases, these patients more often had pulmonary embolism, higher D-dimer levels, and greater use of unfractionated heparin. At 30 days, COVID-19 was associated with increased mortality (HR 2.29; 95% CI 1.19-4.40) and major bleeding (HR 2.11; 95% CI 1.06-4.21). At one year, the bleeding risk remained higher (HR 1.54; 95% CI 1.02-2.33), while VTE recurrence was lower (HR 0.34; 95% CI 0.13-0.94). These results were consistent after propensity score matching. COVID-19-associated VTE is linked to worse short-term outcomes, including early mortality and bleeding, and to a persistently elevated bleeding risk at one year. Lower recurrence rates support the consideration of COVID-19 as a transient provoking factor.</p>","PeriodicalId":13662,"journal":{"name":"Internal and Emergency Medicine","volume":" ","pages":"1835-1846"},"PeriodicalIF":3.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476387/pdf/","citationCount":"0","resultStr":"{\"title\":\"Short and long-term outcomes of COVID-19-associated venous thromboembolism: a propensity score-matched cohort study.\",\"authors\":\"Rubén Alonso-Beato, Pablo Demelo-Rodríguez, Lucía Ordieres-Ortega, Marina López-Rubio, Marta-Olimpia Lago-Rodríguez, Crhistian-Mario Oblitas, Luis Antonio Alvarez-Sala Walther, Francisco Galeano-Valle\",\"doi\":\"10.1007/s11739-025-04042-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Venous thromboembolism (VTE) is a recognized complication of SARS-CoV-2 infection, but its clinical features and both sort- and long-term outcomes remain incompletely characterized. We aimed to compare the clinical profile and outcomes of patients with VTE with and without recent COVID-19. We conducted a prospective cohort study including 2012 patients with objectively confirmed VTE. COVID-19-associated VTE was defined as VTE diagnosed within 30 days of a microbiologically confirmed SARS-CoV-2 infection. Clinical characteristics, treatment, and outcomes were compared between groups. Propensity score matching (1:1) and competing risk models were used to adjust for confounding. The primary outcomes-assessed at both 30 days and 365 days-included all-cause mortality, major bleeding, and VTE recurrence. A total of 272 patients (13.5%) had COVID-19-associated VTE. Compared with non-COVID cases, these patients more often had pulmonary embolism, higher D-dimer levels, and greater use of unfractionated heparin. At 30 days, COVID-19 was associated with increased mortality (HR 2.29; 95% CI 1.19-4.40) and major bleeding (HR 2.11; 95% CI 1.06-4.21). At one year, the bleeding risk remained higher (HR 1.54; 95% CI 1.02-2.33), while VTE recurrence was lower (HR 0.34; 95% CI 0.13-0.94). These results were consistent after propensity score matching. COVID-19-associated VTE is linked to worse short-term outcomes, including early mortality and bleeding, and to a persistently elevated bleeding risk at one year. Lower recurrence rates support the consideration of COVID-19 as a transient provoking factor.</p>\",\"PeriodicalId\":13662,\"journal\":{\"name\":\"Internal and Emergency Medicine\",\"volume\":\" \",\"pages\":\"1835-1846\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476387/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Internal and Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11739-025-04042-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11739-025-04042-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
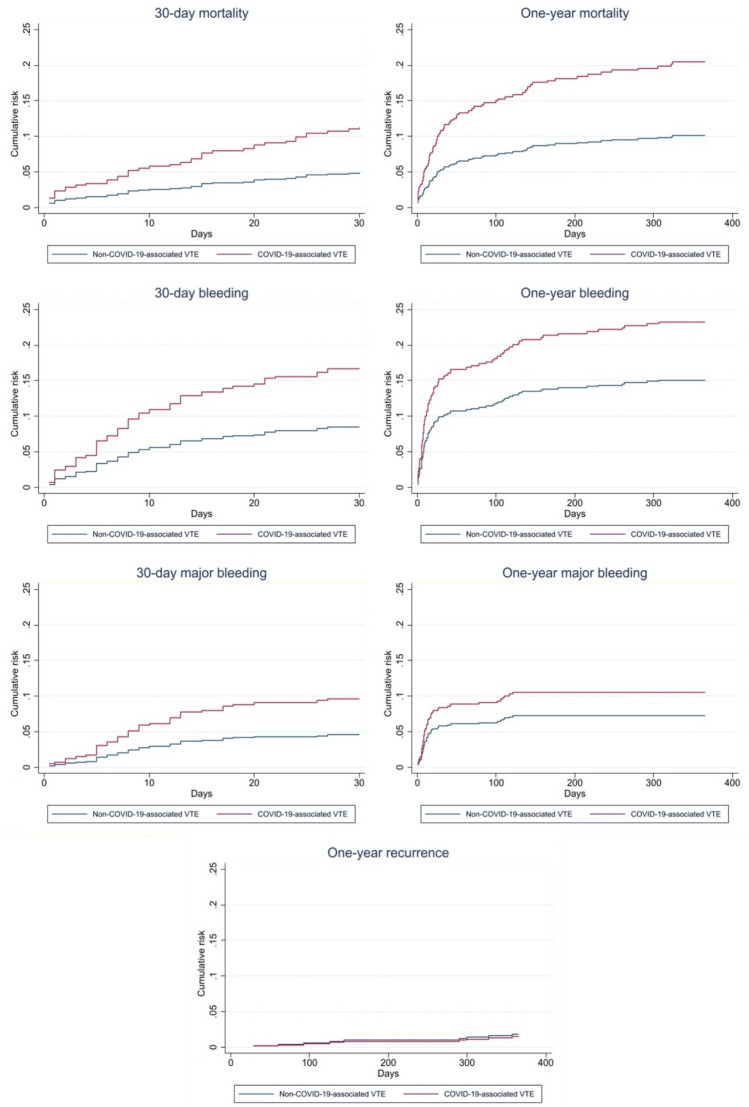
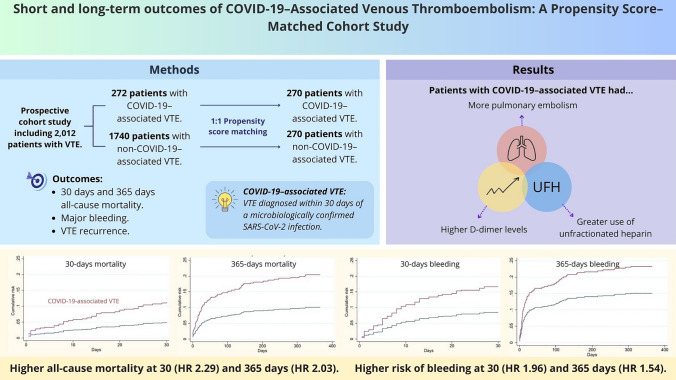
静脉血栓栓塞(VTE)是公认的SARS-CoV-2感染并发症,但其临床特征以及近期和长期结局尚未完全确定。我们的目的是比较近期合并和未合并COVID-19的静脉血栓栓塞患者的临床特征和结局。我们进行了一项前瞻性队列研究,纳入了2012例客观确诊的静脉血栓栓塞患者。与covid -19相关的静脉血栓栓塞被定义为微生物学证实的SARS-CoV-2感染后30天内诊断出的静脉血栓栓塞。比较两组间的临床特征、治疗和结局。倾向得分匹配(1:1)和竞争风险模型用于调整混杂。在30天和365天评估的主要结果包括全因死亡率、大出血和静脉血栓栓塞复发。共有272名患者(13.5%)患有与covid -19相关的静脉血栓栓塞。与非covid病例相比,这些患者更容易发生肺栓塞,d -二聚体水平更高,并且更多地使用未分离肝素。在第30天,COVID-19与死亡率增加相关(HR 2.29;95% CI 1.19-4.40)和大出血(HR 2.11;95% ci 1.06-4.21)。一年后,出血风险仍然较高(HR 1.54;95% CI 1.02-2.33),而静脉血栓栓塞复发率较低(HR 0.34;95% ci 0.13-0.94)。这些结果在倾向评分匹配后是一致的。与covid -19相关的静脉血栓栓塞与更糟糕的短期结果有关,包括早期死亡和出血,并与一年内出血风险持续升高有关。较低的复发率支持将COVID-19视为一种短暂的诱发因素。
Short and long-term outcomes of COVID-19-associated venous thromboembolism: a propensity score-matched cohort study.
Venous thromboembolism (VTE) is a recognized complication of SARS-CoV-2 infection, but its clinical features and both sort- and long-term outcomes remain incompletely characterized. We aimed to compare the clinical profile and outcomes of patients with VTE with and without recent COVID-19. We conducted a prospective cohort study including 2012 patients with objectively confirmed VTE. COVID-19-associated VTE was defined as VTE diagnosed within 30 days of a microbiologically confirmed SARS-CoV-2 infection. Clinical characteristics, treatment, and outcomes were compared between groups. Propensity score matching (1:1) and competing risk models were used to adjust for confounding. The primary outcomes-assessed at both 30 days and 365 days-included all-cause mortality, major bleeding, and VTE recurrence. A total of 272 patients (13.5%) had COVID-19-associated VTE. Compared with non-COVID cases, these patients more often had pulmonary embolism, higher D-dimer levels, and greater use of unfractionated heparin. At 30 days, COVID-19 was associated with increased mortality (HR 2.29; 95% CI 1.19-4.40) and major bleeding (HR 2.11; 95% CI 1.06-4.21). At one year, the bleeding risk remained higher (HR 1.54; 95% CI 1.02-2.33), while VTE recurrence was lower (HR 0.34; 95% CI 0.13-0.94). These results were consistent after propensity score matching. COVID-19-associated VTE is linked to worse short-term outcomes, including early mortality and bleeding, and to a persistently elevated bleeding risk at one year. Lower recurrence rates support the consideration of COVID-19 as a transient provoking factor.
期刊介绍:
Internal and Emergency Medicine (IEM) is an independent, international, English-language, peer-reviewed journal designed for internists and emergency physicians. IEM publishes a variety of manuscript types including Original investigations, Review articles, Letters to the Editor, Editorials and Commentaries. Occasionally IEM accepts unsolicited Reviews, Commentaries or Editorials. The journal is divided into three sections, i.e., Internal Medicine, Emergency Medicine and Clinical Evidence and Health Technology Assessment, with three separate editorial boards. In the Internal Medicine section, invited Case records and Physical examinations, devoted to underlining the role of a clinical approach in selected clinical cases, are also published. The Emergency Medicine section will include a Morbidity and Mortality Report and an Airway Forum concerning the management of difficult airway problems. As far as Critical Care is becoming an integral part of Emergency Medicine, a new sub-section will report the literature that concerns the interface not only for the care of the critical patient in the Emergency Department, but also in the Intensive Care Unit. Finally, in the Clinical Evidence and Health Technology Assessment section brief discussions of topics of evidence-based medicine (Cochrane’s corner) and Research updates are published. IEM encourages letters of rebuttal and criticism of published articles. Topics of interest include all subjects that relate to the science and practice of Internal and Emergency Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


