Manuela Robella, Eva Pagano, Lisa Giacometti, Armando Cinquegrana, Luca Pellegrino, Andrea Evangelista, Alessandra Saliva, Alessandro Cerutti, Felice Borghi
{"title":"在接受细胞减少手术和腹腔内高温化疗的患者中实施增强术后恢复(ERAS)计划:一项前瞻性多中心介入试验(EPICH研究)的研究方案。","authors":"Manuela Robella, Eva Pagano, Lisa Giacometti, Armando Cinquegrana, Luca Pellegrino, Andrea Evangelista, Alessandra Saliva, Alessandro Cerutti, Felice Borghi","doi":"10.1515/pp-2024-0033","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aims to evaluate the clinical impact of introducing an Enhanced Recovery After Surgery (ERAS) protocol in the management of patients undergoing cytoreductive surgery (CRS), with or without hyperthermic intraperitoneal chemotherapy (HIPEC). By addressing a population at high risk of postoperative complications and delayed recovery, the study seeks to determine whether ERAS can improve short-term outcomes, optimize perioperative care, and promote faster and safer recovery in a standardized, evidence-based manner across multiple centers.</p><p><strong>Methods: </strong>The EPICH study is a multicenter, prospective, interventional trial conducted across 20 centers in Italy. A total of 300 patients undergoing CRS±HIPEC will be enrolled in two sequential phases: standard perioperative care followed by ERAS protocol implementation. The primary endpoint is the mean hospital length of stay (LOS). Secondary endpoints include postoperative complications, ICU admission, readmission rates, bowel function recovery, mortality, and patient-reported quality of recovery. The ERAS protocol includes prehabilitation, anemia and nutritional optimization, intraoperative fluid and pain management, and early mobilization and oral feeding. Data will be analyzed using random-effects linear models to account for center-level variation and confounding factors.</p><p><strong>Results: </strong>Preliminary evidence suggests that the ERAS protocol may help reduce mean hospital LOS, postoperative complications, and ICU stays, as well as support faster bowel recovery and improved patient-reported outcomes-findings that this study seeks to validate.</p><p><strong>Conclusions: </strong>The EPICH study could provide robust evidence supporting the adoption of ERAS as the standard of care for patients undergoing CRS±HIPEC, with potential benefits in terms of improved recovery, reduced complications, and decreased healthcare resource utilization.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"10 2","pages":"51-58"},"PeriodicalIF":2.4000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12207391/pdf/","citationCount":"0","resultStr":"{\"title\":\"Implementation of an enhanced recovery after surgery (ERAS) program in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: study protocol for a prospective multicenter interventional trial (EPICH study).\",\"authors\":\"Manuela Robella, Eva Pagano, Lisa Giacometti, Armando Cinquegrana, Luca Pellegrino, Andrea Evangelista, Alessandra Saliva, Alessandro Cerutti, Felice Borghi\",\"doi\":\"10.1515/pp-2024-0033\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>This study aims to evaluate the clinical impact of introducing an Enhanced Recovery After Surgery (ERAS) protocol in the management of patients undergoing cytoreductive surgery (CRS), with or without hyperthermic intraperitoneal chemotherapy (HIPEC). By addressing a population at high risk of postoperative complications and delayed recovery, the study seeks to determine whether ERAS can improve short-term outcomes, optimize perioperative care, and promote faster and safer recovery in a standardized, evidence-based manner across multiple centers.</p><p><strong>Methods: </strong>The EPICH study is a multicenter, prospective, interventional trial conducted across 20 centers in Italy. A total of 300 patients undergoing CRS±HIPEC will be enrolled in two sequential phases: standard perioperative care followed by ERAS protocol implementation. The primary endpoint is the mean hospital length of stay (LOS). Secondary endpoints include postoperative complications, ICU admission, readmission rates, bowel function recovery, mortality, and patient-reported quality of recovery. The ERAS protocol includes prehabilitation, anemia and nutritional optimization, intraoperative fluid and pain management, and early mobilization and oral feeding. Data will be analyzed using random-effects linear models to account for center-level variation and confounding factors.</p><p><strong>Results: </strong>Preliminary evidence suggests that the ERAS protocol may help reduce mean hospital LOS, postoperative complications, and ICU stays, as well as support faster bowel recovery and improved patient-reported outcomes-findings that this study seeks to validate.</p><p><strong>Conclusions: </strong>The EPICH study could provide robust evidence supporting the adoption of ERAS as the standard of care for patients undergoing CRS±HIPEC, with potential benefits in terms of improved recovery, reduced complications, and decreased healthcare resource utilization.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"10 2\",\"pages\":\"51-58\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12207391/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2024-0033\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2024-0033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Implementation of an enhanced recovery after surgery (ERAS) program in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: study protocol for a prospective multicenter interventional trial (EPICH study).
Objectives: This study aims to evaluate the clinical impact of introducing an Enhanced Recovery After Surgery (ERAS) protocol in the management of patients undergoing cytoreductive surgery (CRS), with or without hyperthermic intraperitoneal chemotherapy (HIPEC). By addressing a population at high risk of postoperative complications and delayed recovery, the study seeks to determine whether ERAS can improve short-term outcomes, optimize perioperative care, and promote faster and safer recovery in a standardized, evidence-based manner across multiple centers.
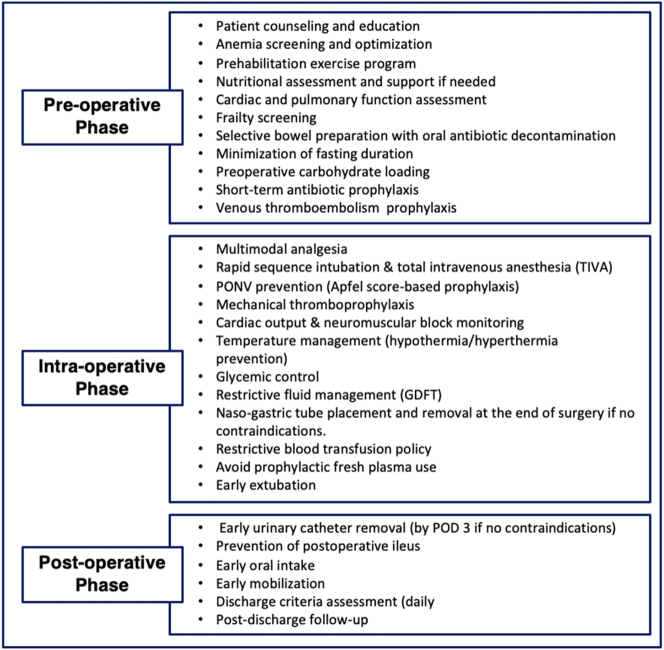
Methods: The EPICH study is a multicenter, prospective, interventional trial conducted across 20 centers in Italy. A total of 300 patients undergoing CRS±HIPEC will be enrolled in two sequential phases: standard perioperative care followed by ERAS protocol implementation. The primary endpoint is the mean hospital length of stay (LOS). Secondary endpoints include postoperative complications, ICU admission, readmission rates, bowel function recovery, mortality, and patient-reported quality of recovery. The ERAS protocol includes prehabilitation, anemia and nutritional optimization, intraoperative fluid and pain management, and early mobilization and oral feeding. Data will be analyzed using random-effects linear models to account for center-level variation and confounding factors.
Results: Preliminary evidence suggests that the ERAS protocol may help reduce mean hospital LOS, postoperative complications, and ICU stays, as well as support faster bowel recovery and improved patient-reported outcomes-findings that this study seeks to validate.
Conclusions: The EPICH study could provide robust evidence supporting the adoption of ERAS as the standard of care for patients undergoing CRS±HIPEC, with potential benefits in terms of improved recovery, reduced complications, and decreased healthcare resource utilization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


