{"title":"ct与超声引导下射频消融治疗膈下肝细胞癌术后复发的比较。","authors":"Hao-Yun Liu, Chih-Yang Hsiao, Rey-Heng Hu, Po-Chin Liang, Chih-Horng Wu","doi":"10.2147/JHC.S524399","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Hepatocellular carcinoma (HCC) remains one of the leading causes of cancer-related mortality worldwide. Although surgical resection and liver transplantation are considered curative, recurrence is common, especially after hepatectomy. Radiofrequency ablation (RFA) offers a minimally invasive alternative for treating recurrent HCC. However, its efficacy is influenced by tumor location and imaging guidance. This study aims to compare the outcomes of CT-guided and US-guided RFA in patients with single small recurrent HCCs located in the subdiaphragmatic region after hepatectomy.</p><p><strong>Methods: </strong>In this retrospective single-center study, we included patients who received RFA for recurrent HCC following curative hepatectomy between 2008 and 2020. Patients were categorized into CT-guided or US-guided RFA groups. RFA was performed by experienced interventional radiologists, and follow-up imaging was conducted every 3-6 months to assess recurrence. The primary outcome was recurrence-free survival (RFS), and the secondary outcome was overall survival (OS).</p><p><strong>Results: </strong>In this study, 59 and 32 patients with subdiaphragmatic lesions underwent CT-guided- and US-guided RFA, respectively, for single recurrent HCC. The CT-guided group showed larger tumor size, lower recurrence rates, and significantly better RFS in Kaplan-Meier analysis compared to the US-guided group (49.5 months vs 35.7 months, p value= 0.042). Multivariate analysis confirmed a superior RFS hazard ratio (HR=0.551) for CT-guided RFA, although the overall survival showed no significant difference. Major complications were absent in both groups.</p><p><strong>Conclusion: </strong>CT-guided RFA provides improved RFS for subdiaphragmatic recurrent HCC, highlighting its potential as a preferred technique for challenging anatomical locations. Further multicenter prospective studies are necessary to validate these findings and assess the long-term survival outcomes.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1231-1240"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212096/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Computed Tomography and Ultrasound-Guided Radiofrequency Ablation for Recurrent Subdiaphragmatic Hepatocellular Carcinoma After Resection.\",\"authors\":\"Hao-Yun Liu, Chih-Yang Hsiao, Rey-Heng Hu, Po-Chin Liang, Chih-Horng Wu\",\"doi\":\"10.2147/JHC.S524399\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Hepatocellular carcinoma (HCC) remains one of the leading causes of cancer-related mortality worldwide. Although surgical resection and liver transplantation are considered curative, recurrence is common, especially after hepatectomy. Radiofrequency ablation (RFA) offers a minimally invasive alternative for treating recurrent HCC. However, its efficacy is influenced by tumor location and imaging guidance. This study aims to compare the outcomes of CT-guided and US-guided RFA in patients with single small recurrent HCCs located in the subdiaphragmatic region after hepatectomy.</p><p><strong>Methods: </strong>In this retrospective single-center study, we included patients who received RFA for recurrent HCC following curative hepatectomy between 2008 and 2020. Patients were categorized into CT-guided or US-guided RFA groups. RFA was performed by experienced interventional radiologists, and follow-up imaging was conducted every 3-6 months to assess recurrence. The primary outcome was recurrence-free survival (RFS), and the secondary outcome was overall survival (OS).</p><p><strong>Results: </strong>In this study, 59 and 32 patients with subdiaphragmatic lesions underwent CT-guided- and US-guided RFA, respectively, for single recurrent HCC. The CT-guided group showed larger tumor size, lower recurrence rates, and significantly better RFS in Kaplan-Meier analysis compared to the US-guided group (49.5 months vs 35.7 months, p value= 0.042). Multivariate analysis confirmed a superior RFS hazard ratio (HR=0.551) for CT-guided RFA, although the overall survival showed no significant difference. Major complications were absent in both groups.</p><p><strong>Conclusion: </strong>CT-guided RFA provides improved RFS for subdiaphragmatic recurrent HCC, highlighting its potential as a preferred technique for challenging anatomical locations. Further multicenter prospective studies are necessary to validate these findings and assess the long-term survival outcomes.</p>\",\"PeriodicalId\":15906,\"journal\":{\"name\":\"Journal of Hepatocellular Carcinoma\",\"volume\":\"12 \",\"pages\":\"1231-1240\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212096/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hepatocellular Carcinoma\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/JHC.S524399\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S524399","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Comparison of Computed Tomography and Ultrasound-Guided Radiofrequency Ablation for Recurrent Subdiaphragmatic Hepatocellular Carcinoma After Resection.
Objective: Hepatocellular carcinoma (HCC) remains one of the leading causes of cancer-related mortality worldwide. Although surgical resection and liver transplantation are considered curative, recurrence is common, especially after hepatectomy. Radiofrequency ablation (RFA) offers a minimally invasive alternative for treating recurrent HCC. However, its efficacy is influenced by tumor location and imaging guidance. This study aims to compare the outcomes of CT-guided and US-guided RFA in patients with single small recurrent HCCs located in the subdiaphragmatic region after hepatectomy.
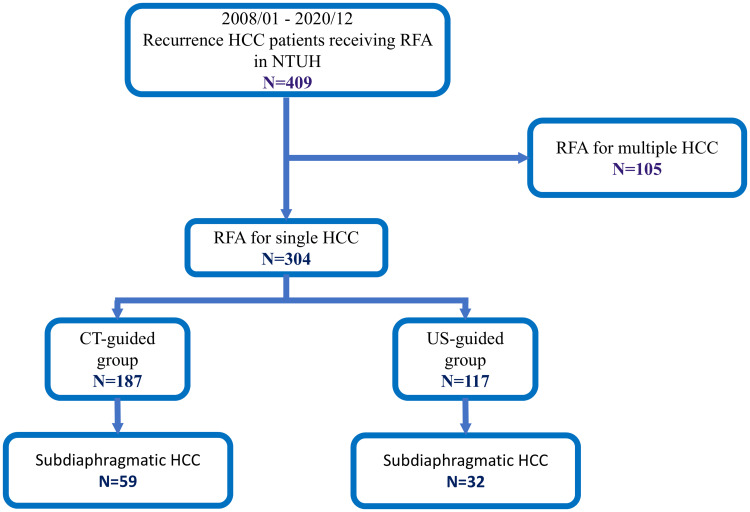
Methods: In this retrospective single-center study, we included patients who received RFA for recurrent HCC following curative hepatectomy between 2008 and 2020. Patients were categorized into CT-guided or US-guided RFA groups. RFA was performed by experienced interventional radiologists, and follow-up imaging was conducted every 3-6 months to assess recurrence. The primary outcome was recurrence-free survival (RFS), and the secondary outcome was overall survival (OS).
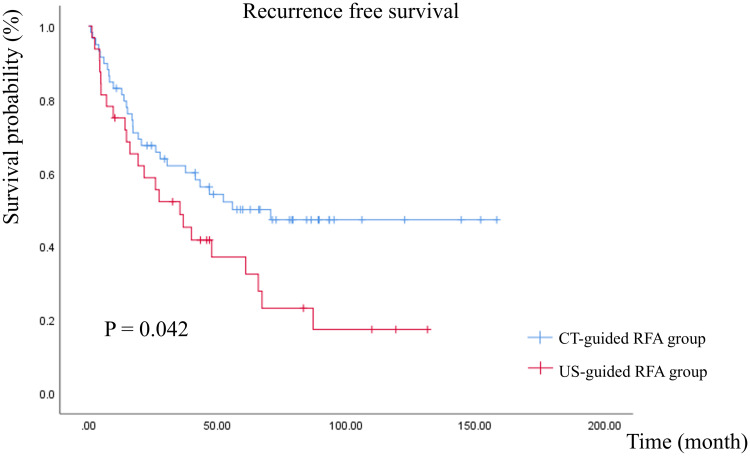
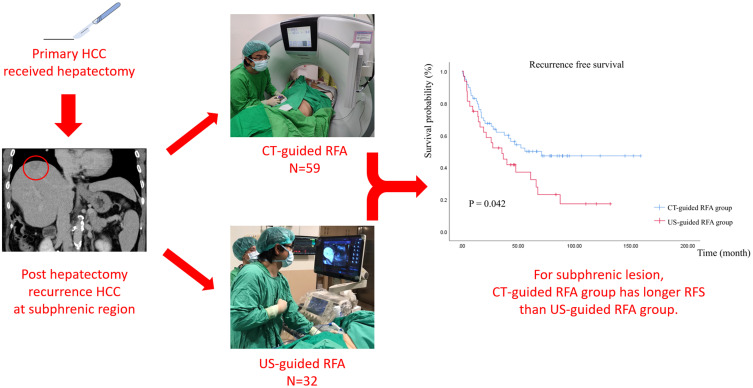
Results: In this study, 59 and 32 patients with subdiaphragmatic lesions underwent CT-guided- and US-guided RFA, respectively, for single recurrent HCC. The CT-guided group showed larger tumor size, lower recurrence rates, and significantly better RFS in Kaplan-Meier analysis compared to the US-guided group (49.5 months vs 35.7 months, p value= 0.042). Multivariate analysis confirmed a superior RFS hazard ratio (HR=0.551) for CT-guided RFA, although the overall survival showed no significant difference. Major complications were absent in both groups.
Conclusion: CT-guided RFA provides improved RFS for subdiaphragmatic recurrent HCC, highlighting its potential as a preferred technique for challenging anatomical locations. Further multicenter prospective studies are necessary to validate these findings and assess the long-term survival outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


