Xiufeng Liu, Lijun Zhuang, Fan Yang, Ping Liu, Zhaojun Xia, Ying Guo, Pingping Dong, Chao Chen, Zixiong Li
{"title":"afp阴性晚期HCC患者的临床结果:来自回顾性队列研究的倾向匹配分析","authors":"Xiufeng Liu, Lijun Zhuang, Fan Yang, Ping Liu, Zhaojun Xia, Ying Guo, Pingping Dong, Chao Chen, Zixiong Li","doi":"10.2147/JHC.S527332","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>AFP positivity (≥20 ng/mL) is often used as one of the diagnostic criteria for HCC. The aim of this study is to analyze the prognosis of advanced HCC with negative (<20 ng/mL) AFP at baseline following systemic drug treatment.</p><p><strong>Methods: </strong>In this study, 91 patients with AFP-negative advanced HCC who received systemic drug treatment in Nanjing Jinling Hospital from February 2011 to September 2023 were collected, and 213 patients with AFP-positive advanced HCC were collected as the control group. A propensity score model was used to adjust for potential confounding variables. Cox regression analysis was used to clarify the differences of prognosis in subgroups for HCC patients.</p><p><strong>Results: </strong>Following propensity score matching with 1:2 ratio, 90 HCC patients from Group A (AFP-negative) and 180 from Group B (AFP-positive) were chosen to participate in the final analysis set. The OS of AFP-negative HCC patients was extended by 13.5 months compared to AFP-positive HCC patients. Within the AFP-negative HCC group, the top-ranked first-line treatment options were TKIs combo ICIs (mPFS = 9.5m, mOS = 37.1m), chemotherapy combo ICIs (mPFS = 8.1m, mOS = 15.5m), and TKIs (mPFS = 5.6m, mOS = 28.2m). Subgroup analysis indicated that among AFP-negative HCC patients, those without PVTT or with HBV DNA <50lU/mL had longer survival time. For HCC patients who opted for TKIs combo ICIs as their first-line treatment and then switched to TKIs alone for second-line treatment, the mOS and 95% CI were 30.7 (24.8-NA) months.</p><p><strong>Conclusion: </strong>The survival time of AFP-negative HCC patients was significantly longer than that of AFP positive HCC patients. Patients with no PVTT or HBV DNA <50lU/mL have relatively better efficacy of systemic drug therapy. With the AFP-negative HCC patients, TKIs combo ICIs are preferentially recommended for the first-line therapy, and TKIs are used for the second-line therapy after progression.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1241-1252"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212435/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes of AFP-Negative Patients with Advanced HCC: A Propensity-Matched Analysis from a Retrospective Cohort Study.\",\"authors\":\"Xiufeng Liu, Lijun Zhuang, Fan Yang, Ping Liu, Zhaojun Xia, Ying Guo, Pingping Dong, Chao Chen, Zixiong Li\",\"doi\":\"10.2147/JHC.S527332\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>AFP positivity (≥20 ng/mL) is often used as one of the diagnostic criteria for HCC. The aim of this study is to analyze the prognosis of advanced HCC with negative (<20 ng/mL) AFP at baseline following systemic drug treatment.</p><p><strong>Methods: </strong>In this study, 91 patients with AFP-negative advanced HCC who received systemic drug treatment in Nanjing Jinling Hospital from February 2011 to September 2023 were collected, and 213 patients with AFP-positive advanced HCC were collected as the control group. A propensity score model was used to adjust for potential confounding variables. Cox regression analysis was used to clarify the differences of prognosis in subgroups for HCC patients.</p><p><strong>Results: </strong>Following propensity score matching with 1:2 ratio, 90 HCC patients from Group A (AFP-negative) and 180 from Group B (AFP-positive) were chosen to participate in the final analysis set. The OS of AFP-negative HCC patients was extended by 13.5 months compared to AFP-positive HCC patients. Within the AFP-negative HCC group, the top-ranked first-line treatment options were TKIs combo ICIs (mPFS = 9.5m, mOS = 37.1m), chemotherapy combo ICIs (mPFS = 8.1m, mOS = 15.5m), and TKIs (mPFS = 5.6m, mOS = 28.2m). Subgroup analysis indicated that among AFP-negative HCC patients, those without PVTT or with HBV DNA <50lU/mL had longer survival time. For HCC patients who opted for TKIs combo ICIs as their first-line treatment and then switched to TKIs alone for second-line treatment, the mOS and 95% CI were 30.7 (24.8-NA) months.</p><p><strong>Conclusion: </strong>The survival time of AFP-negative HCC patients was significantly longer than that of AFP positive HCC patients. Patients with no PVTT or HBV DNA <50lU/mL have relatively better efficacy of systemic drug therapy. With the AFP-negative HCC patients, TKIs combo ICIs are preferentially recommended for the first-line therapy, and TKIs are used for the second-line therapy after progression.</p>\",\"PeriodicalId\":15906,\"journal\":{\"name\":\"Journal of Hepatocellular Carcinoma\",\"volume\":\"12 \",\"pages\":\"1241-1252\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212435/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hepatocellular Carcinoma\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/JHC.S527332\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S527332","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
AFP阳性(≥20 ng/mL)常被作为HCC的诊断标准之一。方法:本研究收集2011年2月至2023年9月在南京金陵医院接受全身药物治疗的afp阴性晚期HCC患者91例,以afp阳性晚期HCC患者213例为对照组。倾向评分模型用于调整潜在的混杂变量。采用Cox回归分析明确HCC患者亚组预后差异。结果:按照1:2比例的倾向评分匹配,选择A组(afp阴性)90例、B组(afp阳性)180例HCC患者参与最终分析集。与afp阳性HCC患者相比,afp阴性HCC患者的生存期延长13.5个月。在afp阴性HCC组中,一线治疗方案排名第一的是TKIs联合ICIs (mPFS = 9.5m, mOS = 371 m)、化疗联合ICIs (mPFS = 8.1m, mOS = 15.5m)和TKIs (mPFS = 5.6m, mOS = 28.2m)。亚组分析显示,在AFP阴性HCC患者中,无PVTT患者和有HBV DNA的HCC患者中,结论:AFP阴性HCC患者的生存时间明显长于AFP阳性HCC患者。没有PVTT或HBV DNA的患者
Clinical Outcomes of AFP-Negative Patients with Advanced HCC: A Propensity-Matched Analysis from a Retrospective Cohort Study.
Introduction: AFP positivity (≥20 ng/mL) is often used as one of the diagnostic criteria for HCC. The aim of this study is to analyze the prognosis of advanced HCC with negative (<20 ng/mL) AFP at baseline following systemic drug treatment.
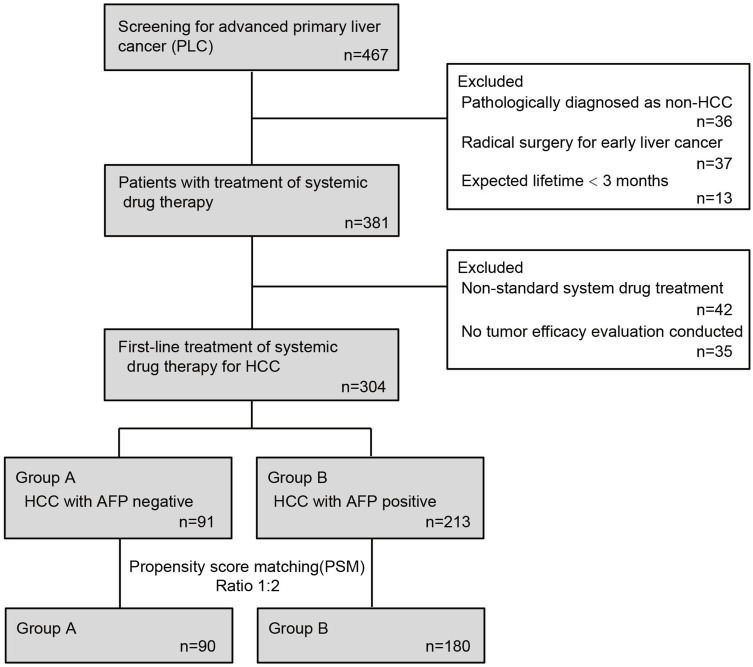
Methods: In this study, 91 patients with AFP-negative advanced HCC who received systemic drug treatment in Nanjing Jinling Hospital from February 2011 to September 2023 were collected, and 213 patients with AFP-positive advanced HCC were collected as the control group. A propensity score model was used to adjust for potential confounding variables. Cox regression analysis was used to clarify the differences of prognosis in subgroups for HCC patients.
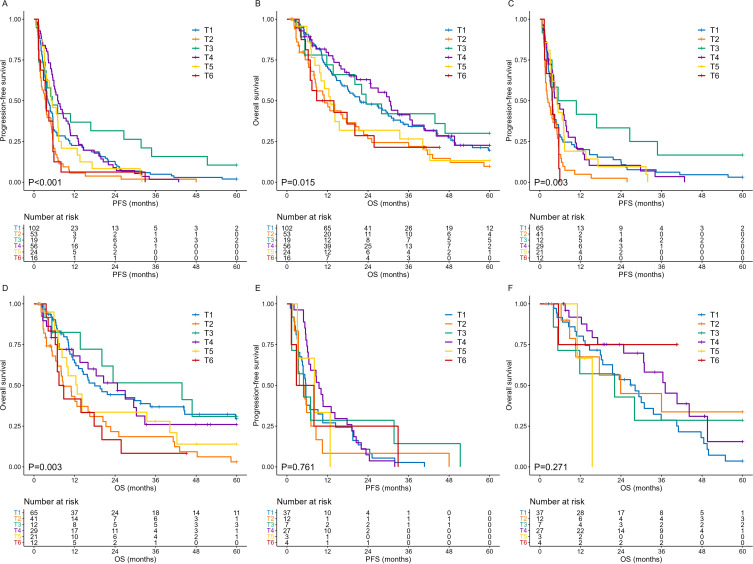
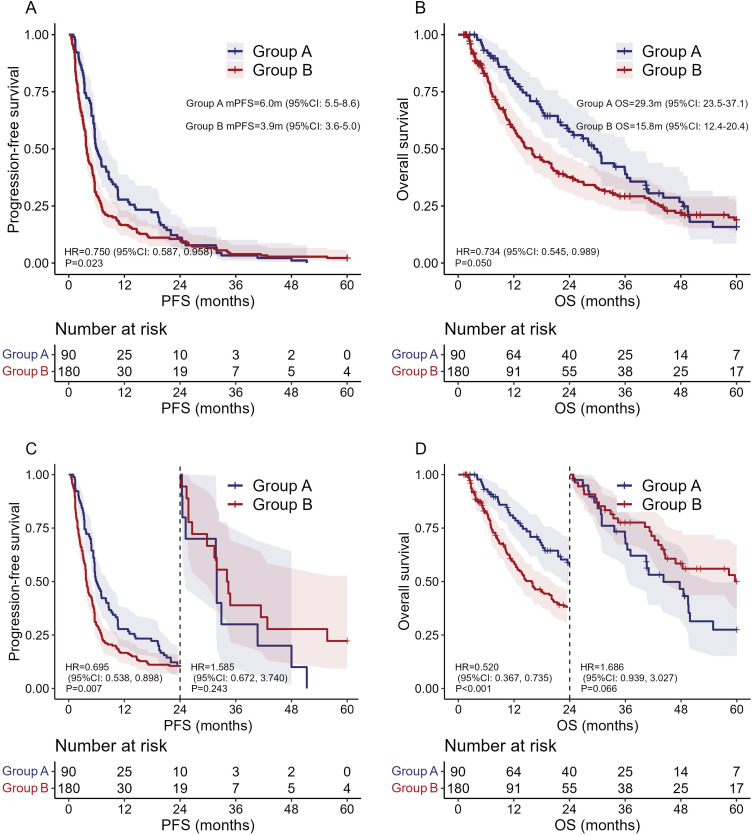
Results: Following propensity score matching with 1:2 ratio, 90 HCC patients from Group A (AFP-negative) and 180 from Group B (AFP-positive) were chosen to participate in the final analysis set. The OS of AFP-negative HCC patients was extended by 13.5 months compared to AFP-positive HCC patients. Within the AFP-negative HCC group, the top-ranked first-line treatment options were TKIs combo ICIs (mPFS = 9.5m, mOS = 37.1m), chemotherapy combo ICIs (mPFS = 8.1m, mOS = 15.5m), and TKIs (mPFS = 5.6m, mOS = 28.2m). Subgroup analysis indicated that among AFP-negative HCC patients, those without PVTT or with HBV DNA <50lU/mL had longer survival time. For HCC patients who opted for TKIs combo ICIs as their first-line treatment and then switched to TKIs alone for second-line treatment, the mOS and 95% CI were 30.7 (24.8-NA) months.
Conclusion: The survival time of AFP-negative HCC patients was significantly longer than that of AFP positive HCC patients. Patients with no PVTT or HBV DNA <50lU/mL have relatively better efficacy of systemic drug therapy. With the AFP-negative HCC patients, TKIs combo ICIs are preferentially recommended for the first-line therapy, and TKIs are used for the second-line therapy after progression.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


