Özlem Kılıç, Seda Çolak, Emre Tekgöz, Mehmet Nur Kaya, Muhammet Çınar, Sedat Yılmaz
{"title":"家族性地中海热发作时,患者会怎么做?他们的策略和相关因素。","authors":"Özlem Kılıç, Seda Çolak, Emre Tekgöz, Mehmet Nur Kaya, Muhammet Çınar, Sedat Yılmaz","doi":"10.1007/s11739-025-04039-6","DOIUrl":null,"url":null,"abstract":"<p><p>Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease characterised by recurrent fever and serositis. Despite colchicine's proven efficacy, attacks may persist, necessitating the implementation of various mitigation strategies by patients. To identify attack mitigation strategies and associated factors in FMF patients. A cross-sectional study at a tertiary rheumatology clinic included adults (≥ 18 years) meeting Tel-Hashomer criteria, on colchicine for ≥ 6 months, with ≥ 1 attack in the past six months. Patients were asked about their attack mitigation strategies, including colchicine dose increase, emergency department (ED) admission, resting, abdominal hot pack, dietary changes, on-demand anakinra, herbs, paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid use. Among 258 patients (98 men, 160 women; median age 35 years, disease duration 18 years), 93% used mitigation strategies. The most common first choice was ED admission (19.8%), followed by colchicine dose increase (18.2%), resting (14.3%), dietary changes (4.3%), NSAIDs (7%), paracetamol (6.6%), on-demand anakinra (6.2%), herbs (6.2%), and corticosteroids (5%). Normal C-reactive protein (CRP) levels, shorter last attack duration, lower international Severity Score for FMF (ISSF), non-working and non-M694V mutations were linked with colchicine dose increase (p < 0.05). M694V positivity, working, persistent CRP elevation, dominant serositis and musculoskeletal attacks, education level ≤ 8 years, longer last attack duration, higher ISSF, current colchicine resistance and non-adherence were linked with ED admission (p < 0.05). Most FMF patients used strategies to mitigate attacks, mainly ED admission and colchicine dose increase. These were influenced by genetic mutations, attack type, working status, education, and CRP levels.</p>","PeriodicalId":13662,"journal":{"name":"Internal and Emergency Medicine","volume":" ","pages":"1823-1833"},"PeriodicalIF":3.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476397/pdf/","citationCount":"0","resultStr":"{\"title\":\"What do patients do during a familial Mediterranean fever attack? Their strategies and associated factors.\",\"authors\":\"Özlem Kılıç, Seda Çolak, Emre Tekgöz, Mehmet Nur Kaya, Muhammet Çınar, Sedat Yılmaz\",\"doi\":\"10.1007/s11739-025-04039-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease characterised by recurrent fever and serositis. Despite colchicine's proven efficacy, attacks may persist, necessitating the implementation of various mitigation strategies by patients. To identify attack mitigation strategies and associated factors in FMF patients. A cross-sectional study at a tertiary rheumatology clinic included adults (≥ 18 years) meeting Tel-Hashomer criteria, on colchicine for ≥ 6 months, with ≥ 1 attack in the past six months. Patients were asked about their attack mitigation strategies, including colchicine dose increase, emergency department (ED) admission, resting, abdominal hot pack, dietary changes, on-demand anakinra, herbs, paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid use. Among 258 patients (98 men, 160 women; median age 35 years, disease duration 18 years), 93% used mitigation strategies. The most common first choice was ED admission (19.8%), followed by colchicine dose increase (18.2%), resting (14.3%), dietary changes (4.3%), NSAIDs (7%), paracetamol (6.6%), on-demand anakinra (6.2%), herbs (6.2%), and corticosteroids (5%). Normal C-reactive protein (CRP) levels, shorter last attack duration, lower international Severity Score for FMF (ISSF), non-working and non-M694V mutations were linked with colchicine dose increase (p < 0.05). M694V positivity, working, persistent CRP elevation, dominant serositis and musculoskeletal attacks, education level ≤ 8 years, longer last attack duration, higher ISSF, current colchicine resistance and non-adherence were linked with ED admission (p < 0.05). Most FMF patients used strategies to mitigate attacks, mainly ED admission and colchicine dose increase. These were influenced by genetic mutations, attack type, working status, education, and CRP levels.</p>\",\"PeriodicalId\":13662,\"journal\":{\"name\":\"Internal and Emergency Medicine\",\"volume\":\" \",\"pages\":\"1823-1833\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476397/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Internal and Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11739-025-04039-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11739-025-04039-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
What do patients do during a familial Mediterranean fever attack? Their strategies and associated factors.
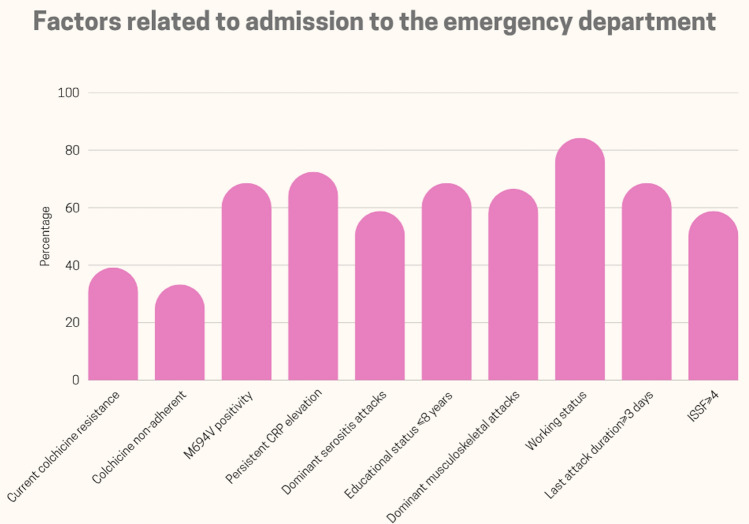
Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease characterised by recurrent fever and serositis. Despite colchicine's proven efficacy, attacks may persist, necessitating the implementation of various mitigation strategies by patients. To identify attack mitigation strategies and associated factors in FMF patients. A cross-sectional study at a tertiary rheumatology clinic included adults (≥ 18 years) meeting Tel-Hashomer criteria, on colchicine for ≥ 6 months, with ≥ 1 attack in the past six months. Patients were asked about their attack mitigation strategies, including colchicine dose increase, emergency department (ED) admission, resting, abdominal hot pack, dietary changes, on-demand anakinra, herbs, paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid use. Among 258 patients (98 men, 160 women; median age 35 years, disease duration 18 years), 93% used mitigation strategies. The most common first choice was ED admission (19.8%), followed by colchicine dose increase (18.2%), resting (14.3%), dietary changes (4.3%), NSAIDs (7%), paracetamol (6.6%), on-demand anakinra (6.2%), herbs (6.2%), and corticosteroids (5%). Normal C-reactive protein (CRP) levels, shorter last attack duration, lower international Severity Score for FMF (ISSF), non-working and non-M694V mutations were linked with colchicine dose increase (p < 0.05). M694V positivity, working, persistent CRP elevation, dominant serositis and musculoskeletal attacks, education level ≤ 8 years, longer last attack duration, higher ISSF, current colchicine resistance and non-adherence were linked with ED admission (p < 0.05). Most FMF patients used strategies to mitigate attacks, mainly ED admission and colchicine dose increase. These were influenced by genetic mutations, attack type, working status, education, and CRP levels.
期刊介绍:
Internal and Emergency Medicine (IEM) is an independent, international, English-language, peer-reviewed journal designed for internists and emergency physicians. IEM publishes a variety of manuscript types including Original investigations, Review articles, Letters to the Editor, Editorials and Commentaries. Occasionally IEM accepts unsolicited Reviews, Commentaries or Editorials. The journal is divided into three sections, i.e., Internal Medicine, Emergency Medicine and Clinical Evidence and Health Technology Assessment, with three separate editorial boards. In the Internal Medicine section, invited Case records and Physical examinations, devoted to underlining the role of a clinical approach in selected clinical cases, are also published. The Emergency Medicine section will include a Morbidity and Mortality Report and an Airway Forum concerning the management of difficult airway problems. As far as Critical Care is becoming an integral part of Emergency Medicine, a new sub-section will report the literature that concerns the interface not only for the care of the critical patient in the Emergency Department, but also in the Intensive Care Unit. Finally, in the Clinical Evidence and Health Technology Assessment section brief discussions of topics of evidence-based medicine (Cochrane’s corner) and Research updates are published. IEM encourages letters of rebuttal and criticism of published articles. Topics of interest include all subjects that relate to the science and practice of Internal and Emergency Medicine.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


