Marta Araujo-Castro, Betina Biagetti, Edelmiro Menéndez, Iría Novoa-Testa, Fernando Cordido, Víctor Rodríguez Berrocal, Eider Pascual-Corrales, Fernando Guerrero-Pérez, Almudena Vicente, Rogelio García-Centeno, Laura González, María Dolores Ollero García, Ana Irigaray Echarri, María Dolores Moure Rodríguez, Cristina Novo-Rodríguez, María Calatayud, Rocío Villar-Taibo, Ignacio Bernabéu, Cristina Alvarez-Escola, Carmen Tenorio Jimenéz, Pablo Abellán-Galiana, Eva Venegas, Inmaculada González-Molero, Pedro Iglesias, Concepción Blanco, Fernando Vidal-Ostos De Lara, María Paz de Miguel Novoa, Elena López-Mezquita Torres, Felicia Hanzu, Cristina Lamas, Silvia Aznar Rodríguez, Anna Aulinas, José María Recio, María Dolores Aviles-Pérez, Miguel Antonio Sampedro Núñez, Rosa Camara, Miguel Paja Fano, Carmen Fajardo, Luís Cardoso, Pedro Marques, Elena Martínez-Sáez, Ignacio Ruz-Caracuel, Mónica Marazuela, Manel Puig-Domingo
{"title":"共同分泌GH和催乳素垂体腺瘤治疗失败的预测因素。","authors":"Marta Araujo-Castro, Betina Biagetti, Edelmiro Menéndez, Iría Novoa-Testa, Fernando Cordido, Víctor Rodríguez Berrocal, Eider Pascual-Corrales, Fernando Guerrero-Pérez, Almudena Vicente, Rogelio García-Centeno, Laura González, María Dolores Ollero García, Ana Irigaray Echarri, María Dolores Moure Rodríguez, Cristina Novo-Rodríguez, María Calatayud, Rocío Villar-Taibo, Ignacio Bernabéu, Cristina Alvarez-Escola, Carmen Tenorio Jimenéz, Pablo Abellán-Galiana, Eva Venegas, Inmaculada González-Molero, Pedro Iglesias, Concepción Blanco, Fernando Vidal-Ostos De Lara, María Paz de Miguel Novoa, Elena López-Mezquita Torres, Felicia Hanzu, Cristina Lamas, Silvia Aznar Rodríguez, Anna Aulinas, José María Recio, María Dolores Aviles-Pérez, Miguel Antonio Sampedro Núñez, Rosa Camara, Miguel Paja Fano, Carmen Fajardo, Luís Cardoso, Pedro Marques, Elena Martínez-Sáez, Ignacio Ruz-Caracuel, Mónica Marazuela, Manel Puig-Domingo","doi":"10.1530/EC-25-0103","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To evaluate which factors are associated with a higher probability of failure to surgical and first-generation somatostatin receptor ligands (fgSRLs) treatment in patients with growth hormone and prolactin co-secreting pituitary adenomas (GH&PRL-PAs).</p><p><strong>Methods: </strong>Acromegaly patients with GH&PRL-PAs included in the ACRO-SPAIN study were enrolled. GH&PRL-PAs were defined as tumors with serum PRL levels above the upper limit of normal and positive immunostaining for GH and PRL, or with PRL levels ≥100 ng/mL when immunostaining data were not available.</p><p><strong>Results: </strong>A total of 126 acromegaly patients with GH&PRL-PAs who underwent transsphenoidal pituitary surgery were included, and 42.1% (n = 53) were biochemically cured at the immediate postoperative evaluation. Knosp grade >2 (odds ratio (OR) 3.48, 95% CI 1.28-9.38), higher serum GH (OR 1.01, 95% CI 1.01-1.08) and IGF-1 (OR 1.60, 95% CI 1.05-2.45) levels were associated with a lower probability of surgical cure. Sixty-eight patients received first-line medical therapy as follows: fgSRLs in monotherapy (n = 22), fgSRL plus cabergoline (n = 37), cabergoline in monotherapy (n = 7) and pegvisomant in monotherapy (n = 2). Among the cases treated with fgSRL in monotherapy, 18.2% (n = 4/22) were resistant. We identified as predictors of fgSRL resistance (in monotherapy and combined with cabergoline) a Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031) and higher postoperative GH levels (OR 1.05, P = 0.006), but no predictors of response to fgSRL in monotherapy were identified.</p><p><strong>Conclusion: </strong>The clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL, co-secretion.</p><p><strong>Significance statement: </strong>In this article focused on GH&PRL pituitary adenomas, we found that a Knosp grade >2, and higher serum GH and IGF-1 levels were associated with a lower probability of surgical cure in these tumors. Regarding the response to fgSRL in monotherapy, 18% of the patients with GH&PRL pituitary adenomas were classified as resistant. Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031), and higher postoperative GH levels (OR 1.05, P = 0.006) were predictors of non-response to fgSRL (monotherapy or combined with cabergoline), while no predictors of response to fgSRL in monotherapy were identified. Thus, we concluded the clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL co-secretion.</p>","PeriodicalId":11634,"journal":{"name":"Endocrine Connections","volume":" ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12268987/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors of therapeutic failure in GH and prolactin co-secreting pituitary adenomas.\",\"authors\":\"Marta Araujo-Castro, Betina Biagetti, Edelmiro Menéndez, Iría Novoa-Testa, Fernando Cordido, Víctor Rodríguez Berrocal, Eider Pascual-Corrales, Fernando Guerrero-Pérez, Almudena Vicente, Rogelio García-Centeno, Laura González, María Dolores Ollero García, Ana Irigaray Echarri, María Dolores Moure Rodríguez, Cristina Novo-Rodríguez, María Calatayud, Rocío Villar-Taibo, Ignacio Bernabéu, Cristina Alvarez-Escola, Carmen Tenorio Jimenéz, Pablo Abellán-Galiana, Eva Venegas, Inmaculada González-Molero, Pedro Iglesias, Concepción Blanco, Fernando Vidal-Ostos De Lara, María Paz de Miguel Novoa, Elena López-Mezquita Torres, Felicia Hanzu, Cristina Lamas, Silvia Aznar Rodríguez, Anna Aulinas, José María Recio, María Dolores Aviles-Pérez, Miguel Antonio Sampedro Núñez, Rosa Camara, Miguel Paja Fano, Carmen Fajardo, Luís Cardoso, Pedro Marques, Elena Martínez-Sáez, Ignacio Ruz-Caracuel, Mónica Marazuela, Manel Puig-Domingo\",\"doi\":\"10.1530/EC-25-0103\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To evaluate which factors are associated with a higher probability of failure to surgical and first-generation somatostatin receptor ligands (fgSRLs) treatment in patients with growth hormone and prolactin co-secreting pituitary adenomas (GH&PRL-PAs).</p><p><strong>Methods: </strong>Acromegaly patients with GH&PRL-PAs included in the ACRO-SPAIN study were enrolled. GH&PRL-PAs were defined as tumors with serum PRL levels above the upper limit of normal and positive immunostaining for GH and PRL, or with PRL levels ≥100 ng/mL when immunostaining data were not available.</p><p><strong>Results: </strong>A total of 126 acromegaly patients with GH&PRL-PAs who underwent transsphenoidal pituitary surgery were included, and 42.1% (n = 53) were biochemically cured at the immediate postoperative evaluation. Knosp grade >2 (odds ratio (OR) 3.48, 95% CI 1.28-9.38), higher serum GH (OR 1.01, 95% CI 1.01-1.08) and IGF-1 (OR 1.60, 95% CI 1.05-2.45) levels were associated with a lower probability of surgical cure. Sixty-eight patients received first-line medical therapy as follows: fgSRLs in monotherapy (n = 22), fgSRL plus cabergoline (n = 37), cabergoline in monotherapy (n = 7) and pegvisomant in monotherapy (n = 2). Among the cases treated with fgSRL in monotherapy, 18.2% (n = 4/22) were resistant. We identified as predictors of fgSRL resistance (in monotherapy and combined with cabergoline) a Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031) and higher postoperative GH levels (OR 1.05, P = 0.006), but no predictors of response to fgSRL in monotherapy were identified.</p><p><strong>Conclusion: </strong>The clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL, co-secretion.</p><p><strong>Significance statement: </strong>In this article focused on GH&PRL pituitary adenomas, we found that a Knosp grade >2, and higher serum GH and IGF-1 levels were associated with a lower probability of surgical cure in these tumors. Regarding the response to fgSRL in monotherapy, 18% of the patients with GH&PRL pituitary adenomas were classified as resistant. Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031), and higher postoperative GH levels (OR 1.05, P = 0.006) were predictors of non-response to fgSRL (monotherapy or combined with cabergoline), while no predictors of response to fgSRL in monotherapy were identified. Thus, we concluded the clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL co-secretion.</p>\",\"PeriodicalId\":11634,\"journal\":{\"name\":\"Endocrine Connections\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12268987/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine Connections\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1530/EC-25-0103\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine Connections","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/EC-25-0103","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Print","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Predictors of therapeutic failure in GH and prolactin co-secreting pituitary adenomas.
Aim: To evaluate which factors are associated with a higher probability of failure to surgical and first-generation somatostatin receptor ligands (fgSRLs) treatment in patients with growth hormone and prolactin co-secreting pituitary adenomas (GH&PRL-PAs).
Methods: Acromegaly patients with GH&PRL-PAs included in the ACRO-SPAIN study were enrolled. GH&PRL-PAs were defined as tumors with serum PRL levels above the upper limit of normal and positive immunostaining for GH and PRL, or with PRL levels ≥100 ng/mL when immunostaining data were not available.
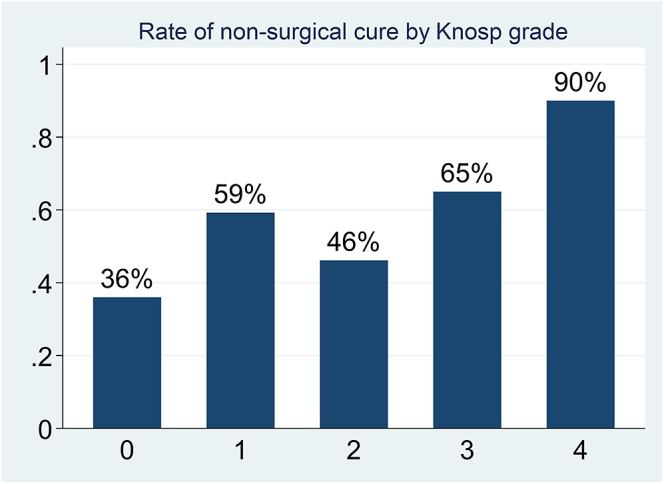
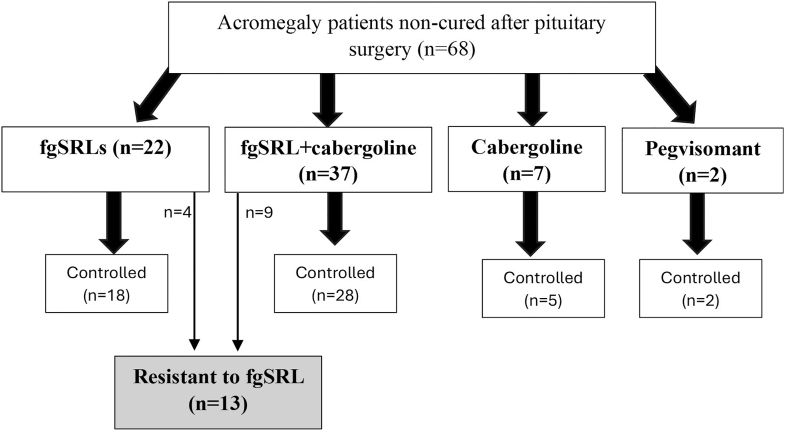
Results: A total of 126 acromegaly patients with GH&PRL-PAs who underwent transsphenoidal pituitary surgery were included, and 42.1% (n = 53) were biochemically cured at the immediate postoperative evaluation. Knosp grade >2 (odds ratio (OR) 3.48, 95% CI 1.28-9.38), higher serum GH (OR 1.01, 95% CI 1.01-1.08) and IGF-1 (OR 1.60, 95% CI 1.05-2.45) levels were associated with a lower probability of surgical cure. Sixty-eight patients received first-line medical therapy as follows: fgSRLs in monotherapy (n = 22), fgSRL plus cabergoline (n = 37), cabergoline in monotherapy (n = 7) and pegvisomant in monotherapy (n = 2). Among the cases treated with fgSRL in monotherapy, 18.2% (n = 4/22) were resistant. We identified as predictors of fgSRL resistance (in monotherapy and combined with cabergoline) a Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031) and higher postoperative GH levels (OR 1.05, P = 0.006), but no predictors of response to fgSRL in monotherapy were identified.
Conclusion: The clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL, co-secretion.
Significance statement: In this article focused on GH&PRL pituitary adenomas, we found that a Knosp grade >2, and higher serum GH and IGF-1 levels were associated with a lower probability of surgical cure in these tumors. Regarding the response to fgSRL in monotherapy, 18% of the patients with GH&PRL pituitary adenomas were classified as resistant. Knosp grade >2 (OR 8.75, P = 0.003), high GH levels at acromegaly diagnosis (OR 1.02, P = 0.031), and higher postoperative GH levels (OR 1.05, P = 0.006) were predictors of non-response to fgSRL (monotherapy or combined with cabergoline), while no predictors of response to fgSRL in monotherapy were identified. Thus, we concluded the clinical predictors of surgical failure and of fgSRL resistance in patients with GH&PRL-PAs are similar to those described in acromegaly without PRL co-secretion.
期刊介绍:
Endocrine Connections publishes original quality research and reviews in all areas of endocrinology, including papers that deal with non-classical tissues as source or targets of hormones and endocrine papers that have relevance to endocrine-related and intersecting disciplines and the wider biomedical community.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


