{"title":"原发性1型高血氧症患儿奈多西兰临床开发和剂量指导的人群药代动力学和药效学建模与模拟。","authors":"Steven Zhang, Pablo Gamallo, Verity Rawson","doi":"10.1007/s40262-025-01540-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Nedosiran (Rivfloza<sup>®</sup>) is an RNA interference (RNAi) therapy approved for individuals aged ≥ 2 years with primary hyperoxaluria type 1 (PH1), a rare autosomal-recessive disorder causing renal failure and systemic oxalosis. Nedosiran silences lactate dehydrogenase (LDH) mRNA in hepatocytes, reducing oxalate levels. This study evaluated the model-informed clinical development of nedosiran to support proposed doses in children aged 2 to < 12 years with PH1.</p><p><strong>Methods: </strong>A population pharmacokinetic/pharmacodynamic (Pop-PK/PD) model characterizing the plasma concentration-time profile of nedosiran and its effect on the spot urine oxalate-to-creatinine ratio (Uox/Cr) was developed using data from six trials. Simulations assessed spot Uox/Cr reduction in children aged 2 to < 12 years for the proposed dosing regimen versus those aged ≥ 12 years weighing ≥ 50 kg with similar renal function.</p><p><strong>Results: </strong>The datasets included 2087 PK (N = 148) and 668 spot Uox/Cr (N = 41, with PH1) observations. Body weight, estimated glomerular filtration rate (eGFR), and PH type were covariates in the PK model, with body weight in low and high percentiles affecting nedosiran exposures. Moderate renal impairment (eGFR 30-59 mL/min/1.73 m<sup>2</sup>) increased exposure, while only age was significant for baseline Uox/Cr in the PD model. Simulations showed similar Uox/Cr reduction and times to maximum effect in children aged 2 to < 12 years, treated once-monthly (Q1M) with 3.5 mg/kg, compared to those aged ≥ 12 years treated Q1M with 170 mg.</p><p><strong>Conclusions: </strong>Simulations based on the final Pop-PK/PD model support the 3.5 mg/kg Q1M dosing regimen in children aged 2 to < 12 years with PH1 and relatively intact kidney function (eGFR ≥30 mL/min/1.73 m<sup>2</sup>).</p><p><strong>Trial registration: </strong>Trials are registered at ClinicalTrials.gov with study numbers NCT03392896 (PHYOX1), NCT03847909 (PHYOX2), NCT04042402 (PHYOX3), and NCT05001269 (PHYOX8) and at EudraCT with study numbers 2018-003098-91 (PHYOX2) and 2018-003099-10 (PHYOX3).</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"1395-1411"},"PeriodicalIF":4.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414044/pdf/","citationCount":"0","resultStr":"{\"title\":\"Population Pharmacokinetic and Pharmacodynamic Modelling and Simulation for Nedosiran Clinical Development and Dose Guidance in Pediatric Patients with Primary Hyperoxaluria Type 1.\",\"authors\":\"Steven Zhang, Pablo Gamallo, Verity Rawson\",\"doi\":\"10.1007/s40262-025-01540-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Nedosiran (Rivfloza<sup>®</sup>) is an RNA interference (RNAi) therapy approved for individuals aged ≥ 2 years with primary hyperoxaluria type 1 (PH1), a rare autosomal-recessive disorder causing renal failure and systemic oxalosis. Nedosiran silences lactate dehydrogenase (LDH) mRNA in hepatocytes, reducing oxalate levels. This study evaluated the model-informed clinical development of nedosiran to support proposed doses in children aged 2 to < 12 years with PH1.</p><p><strong>Methods: </strong>A population pharmacokinetic/pharmacodynamic (Pop-PK/PD) model characterizing the plasma concentration-time profile of nedosiran and its effect on the spot urine oxalate-to-creatinine ratio (Uox/Cr) was developed using data from six trials. Simulations assessed spot Uox/Cr reduction in children aged 2 to < 12 years for the proposed dosing regimen versus those aged ≥ 12 years weighing ≥ 50 kg with similar renal function.</p><p><strong>Results: </strong>The datasets included 2087 PK (N = 148) and 668 spot Uox/Cr (N = 41, with PH1) observations. Body weight, estimated glomerular filtration rate (eGFR), and PH type were covariates in the PK model, with body weight in low and high percentiles affecting nedosiran exposures. Moderate renal impairment (eGFR 30-59 mL/min/1.73 m<sup>2</sup>) increased exposure, while only age was significant for baseline Uox/Cr in the PD model. Simulations showed similar Uox/Cr reduction and times to maximum effect in children aged 2 to < 12 years, treated once-monthly (Q1M) with 3.5 mg/kg, compared to those aged ≥ 12 years treated Q1M with 170 mg.</p><p><strong>Conclusions: </strong>Simulations based on the final Pop-PK/PD model support the 3.5 mg/kg Q1M dosing regimen in children aged 2 to < 12 years with PH1 and relatively intact kidney function (eGFR ≥30 mL/min/1.73 m<sup>2</sup>).</p><p><strong>Trial registration: </strong>Trials are registered at ClinicalTrials.gov with study numbers NCT03392896 (PHYOX1), NCT03847909 (PHYOX2), NCT04042402 (PHYOX3), and NCT05001269 (PHYOX8) and at EudraCT with study numbers 2018-003098-91 (PHYOX2) and 2018-003099-10 (PHYOX3).</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":\" \",\"pages\":\"1395-1411\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414044/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-025-01540-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01540-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Population Pharmacokinetic and Pharmacodynamic Modelling and Simulation for Nedosiran Clinical Development and Dose Guidance in Pediatric Patients with Primary Hyperoxaluria Type 1.
Background and objectives: Nedosiran (Rivfloza®) is an RNA interference (RNAi) therapy approved for individuals aged ≥ 2 years with primary hyperoxaluria type 1 (PH1), a rare autosomal-recessive disorder causing renal failure and systemic oxalosis. Nedosiran silences lactate dehydrogenase (LDH) mRNA in hepatocytes, reducing oxalate levels. This study evaluated the model-informed clinical development of nedosiran to support proposed doses in children aged 2 to < 12 years with PH1.
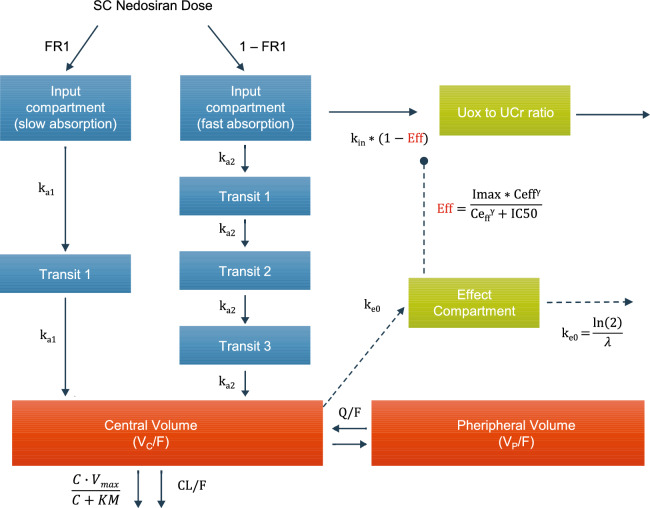
Methods: A population pharmacokinetic/pharmacodynamic (Pop-PK/PD) model characterizing the plasma concentration-time profile of nedosiran and its effect on the spot urine oxalate-to-creatinine ratio (Uox/Cr) was developed using data from six trials. Simulations assessed spot Uox/Cr reduction in children aged 2 to < 12 years for the proposed dosing regimen versus those aged ≥ 12 years weighing ≥ 50 kg with similar renal function.
Results: The datasets included 2087 PK (N = 148) and 668 spot Uox/Cr (N = 41, with PH1) observations. Body weight, estimated glomerular filtration rate (eGFR), and PH type were covariates in the PK model, with body weight in low and high percentiles affecting nedosiran exposures. Moderate renal impairment (eGFR 30-59 mL/min/1.73 m2) increased exposure, while only age was significant for baseline Uox/Cr in the PD model. Simulations showed similar Uox/Cr reduction and times to maximum effect in children aged 2 to < 12 years, treated once-monthly (Q1M) with 3.5 mg/kg, compared to those aged ≥ 12 years treated Q1M with 170 mg.
Conclusions: Simulations based on the final Pop-PK/PD model support the 3.5 mg/kg Q1M dosing regimen in children aged 2 to < 12 years with PH1 and relatively intact kidney function (eGFR ≥30 mL/min/1.73 m2).
Trial registration: Trials are registered at ClinicalTrials.gov with study numbers NCT03392896 (PHYOX1), NCT03847909 (PHYOX2), NCT04042402 (PHYOX3), and NCT05001269 (PHYOX8) and at EudraCT with study numbers 2018-003098-91 (PHYOX2) and 2018-003099-10 (PHYOX3).
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


