Sandhir B Prasad, Liam Scanlon, Anish Krishnan, Nicole Ivy Chan, Michael Mallouhi, William Vollbon, William Parsonage, Sankalp Khanna, Andrew Lin, John J Atherton
{"title":"机器学习整合超声心动图和临床数据,提高心肌梗死后生存预测。","authors":"Sandhir B Prasad, Liam Scanlon, Anish Krishnan, Nicole Ivy Chan, Michael Mallouhi, William Vollbon, William Parsonage, Sankalp Khanna, Andrew Lin, John J Atherton","doi":"10.1093/ehjopen/oeaf064","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Machine learning (ML) could improve risk stratification following myocardial infarction (MI). However, previous ML studies for risk prediction following MI did not incorporate comprehensive echocardiographic data. This study sought to use machine learning (ML) to integrate comprehensive echocardiographic and clinical data for the predicting all-cause mortality following MI.</p><p><strong>Methods and results: </strong>Retrospective study of consecutive patients admitted with MI to a tertiary referral hospital, with echocardiography performed within 24 h of admission. The cohort was randomly split into training (70%) and test (30%) sets. Two ML models (XGBoost and a neural network) were developed using echocardiographic and clinical data, and then compared with conventional logistic regression. The Shapley Additive exPlanations method was used for ML model interpretation. In the final study population of 3202 patients (mean age, 63.2 ± 12.5 years; 29.2% females), ST-elevation MI was present in 28.8%, and the mean cohort LVEF was 52.5 ± 11.2%. At a median follow-up of 4.5 years, there were 465 deaths. In the test set, XGBoost achieved the highest performance (AUC, 0.854), compared with logistic regression (AUC, 0.824; <i>P</i> = 0.006) and the neural network (AUC, 0.808; <i>P</i> = <0.001) for the prediction of death. In the XGBoost model, the highest-ranked predictors included age, renal function, echocardiographic left ventricular outflow velocity time integral, and diastolic parameters. Further, in nested ML models, the addition of echocardiographic parameters provided incremental value beyond clinical variables alone (AUC, 0.854 vs. 0.820; <i>P</i> = 0.002).</p><p><strong>Conclusion: </strong>ML integration of comprehensive echocardiographic data with clinical data could lead to improved prediction of survival following MI. Clinical implementation should be considered.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf064"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12203351/pdf/","citationCount":"0","resultStr":"{\"title\":\"Machine learning integration of echocardiographic and clinical data to improve prediction of survival following myocardial infarction.\",\"authors\":\"Sandhir B Prasad, Liam Scanlon, Anish Krishnan, Nicole Ivy Chan, Michael Mallouhi, William Vollbon, William Parsonage, Sankalp Khanna, Andrew Lin, John J Atherton\",\"doi\":\"10.1093/ehjopen/oeaf064\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Machine learning (ML) could improve risk stratification following myocardial infarction (MI). However, previous ML studies for risk prediction following MI did not incorporate comprehensive echocardiographic data. This study sought to use machine learning (ML) to integrate comprehensive echocardiographic and clinical data for the predicting all-cause mortality following MI.</p><p><strong>Methods and results: </strong>Retrospective study of consecutive patients admitted with MI to a tertiary referral hospital, with echocardiography performed within 24 h of admission. The cohort was randomly split into training (70%) and test (30%) sets. Two ML models (XGBoost and a neural network) were developed using echocardiographic and clinical data, and then compared with conventional logistic regression. The Shapley Additive exPlanations method was used for ML model interpretation. In the final study population of 3202 patients (mean age, 63.2 ± 12.5 years; 29.2% females), ST-elevation MI was present in 28.8%, and the mean cohort LVEF was 52.5 ± 11.2%. At a median follow-up of 4.5 years, there were 465 deaths. In the test set, XGBoost achieved the highest performance (AUC, 0.854), compared with logistic regression (AUC, 0.824; <i>P</i> = 0.006) and the neural network (AUC, 0.808; <i>P</i> = <0.001) for the prediction of death. In the XGBoost model, the highest-ranked predictors included age, renal function, echocardiographic left ventricular outflow velocity time integral, and diastolic parameters. Further, in nested ML models, the addition of echocardiographic parameters provided incremental value beyond clinical variables alone (AUC, 0.854 vs. 0.820; <i>P</i> = 0.002).</p><p><strong>Conclusion: </strong>ML integration of comprehensive echocardiographic data with clinical data could lead to improved prediction of survival following MI. Clinical implementation should be considered.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf064\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12203351/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf064\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:机器学习(ML)可以改善心肌梗死(MI)后的风险分层。然而,先前用于心肌梗死后风险预测的ML研究并没有纳入全面的超声心动图数据。本研究试图利用机器学习(ML)整合全面的超声心动图和临床数据,以预测心肌梗死后的全因死亡率。方法和结果:回顾性研究连续入住三级转诊医院的心肌梗死患者,入院后24小时内进行超声心动图检查。队列随机分为训练组(70%)和测试组(30%)。利用超声心动图和临床数据建立两种ML模型(XGBoost和神经网络),并与常规逻辑回归进行比较。ML模型解释采用Shapley加性解释方法。最终研究人群为3202例患者(平均年龄63.2±12.5岁;29.2%的女性),28.8%的患者存在st段抬高性心肌梗死,平均队列LVEF为52.5±11.2%。在平均4.5年的随访中,有465人死亡。在测试集中,XGBoost取得了最高的性能(AUC, 0.854),而逻辑回归(AUC, 0.824;P = 0.006)和神经网络(AUC, 0.808;P = P = 0.002)。结论:综合超声心动图资料与临床资料的ML整合可提高心肌梗死后的生存预测,应考虑临床应用。
Machine learning integration of echocardiographic and clinical data to improve prediction of survival following myocardial infarction.
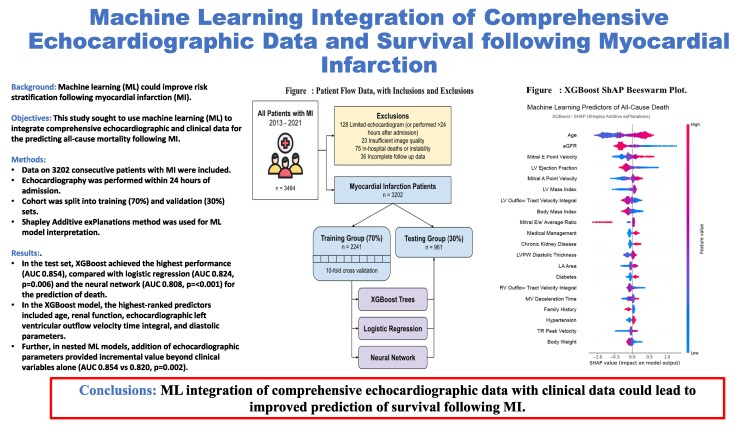
Aims: Machine learning (ML) could improve risk stratification following myocardial infarction (MI). However, previous ML studies for risk prediction following MI did not incorporate comprehensive echocardiographic data. This study sought to use machine learning (ML) to integrate comprehensive echocardiographic and clinical data for the predicting all-cause mortality following MI.
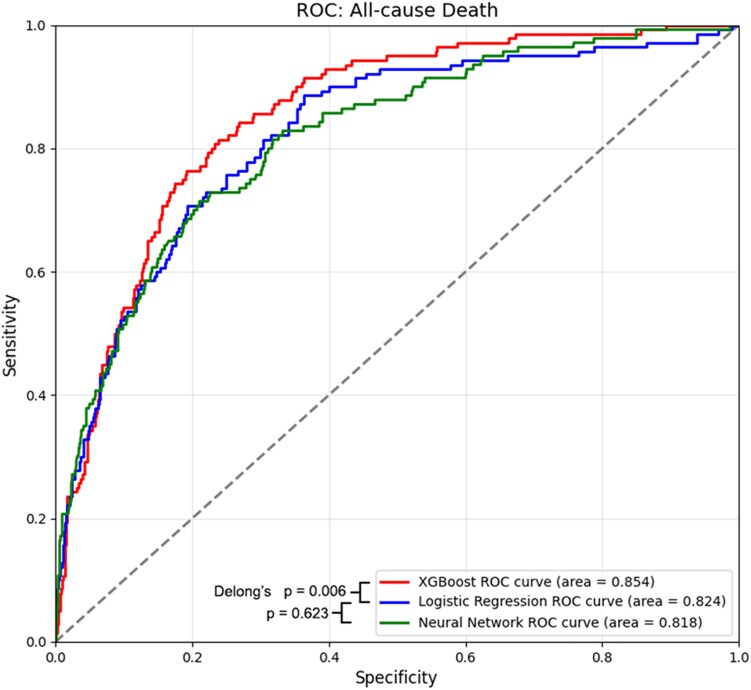
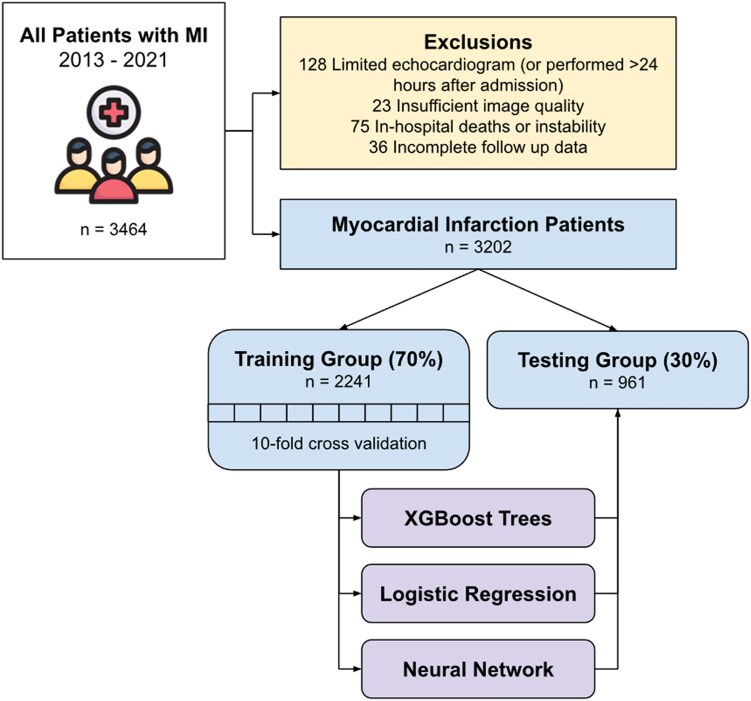
Methods and results: Retrospective study of consecutive patients admitted with MI to a tertiary referral hospital, with echocardiography performed within 24 h of admission. The cohort was randomly split into training (70%) and test (30%) sets. Two ML models (XGBoost and a neural network) were developed using echocardiographic and clinical data, and then compared with conventional logistic regression. The Shapley Additive exPlanations method was used for ML model interpretation. In the final study population of 3202 patients (mean age, 63.2 ± 12.5 years; 29.2% females), ST-elevation MI was present in 28.8%, and the mean cohort LVEF was 52.5 ± 11.2%. At a median follow-up of 4.5 years, there were 465 deaths. In the test set, XGBoost achieved the highest performance (AUC, 0.854), compared with logistic regression (AUC, 0.824; P = 0.006) and the neural network (AUC, 0.808; P = <0.001) for the prediction of death. In the XGBoost model, the highest-ranked predictors included age, renal function, echocardiographic left ventricular outflow velocity time integral, and diastolic parameters. Further, in nested ML models, the addition of echocardiographic parameters provided incremental value beyond clinical variables alone (AUC, 0.854 vs. 0.820; P = 0.002).
Conclusion: ML integration of comprehensive echocardiographic data with clinical data could lead to improved prediction of survival following MI. Clinical implementation should be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


