Omar Bushara, Yash Kadakia, Katharine Krupp, Jessica Friedman, Maarouf A Hoteit, Therese Bittermann, Tarek Araji, Matthew H Levine
{"title":"中心经验与肝门部胆管癌肝移植生存率提高相关:一项回顾性研究。","authors":"Omar Bushara, Yash Kadakia, Katharine Krupp, Jessica Friedman, Maarouf A Hoteit, Therese Bittermann, Tarek Araji, Matthew H Levine","doi":"10.1097/TXD.0000000000001822","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hilar cholangiocarcinoma has limited treatments, with transplantation emerging as a curative option. During the era of regional patient review, it was suggested that transplant centers performing a higher volume of transplants for cholangiocarcinoma had improved outcomes. However, it is unknown whether this association persists since the national standardization of guidelines in May 2019.</p><p><strong>Methods: </strong>Transplant candidates listed in the United Network of Organ Sharing database using cholangiocarcinoma exception points from May 2019 to December 2022 were included. Experienced centers were defined as performing at least 10 transplants during the time period. Recipient and donor characteristics, graft and patient survival, and hospital length of stay were compared between more and less experienced centers. The Wilcoxon rank-sum test, Fisher exact test, Kaplan-Meier curves, log-rank tests, and Cox hazards analyses were used where appropriate.</p><p><strong>Results: </strong>Between May 2019 and December 2022, 166 transplants for cholangiocarcinoma were performed at 37 centers, with \"more experienced\" centers accounting for 59% (n = 98). Unadjusted graft survival (<i>P</i> = 0.03) and patient survival (<i>P</i> = 0.047) were lower at less experienced centers. In addition to center experience, univariable Cox analyses recipient age (0.02), diabetes (0.18), and donor age (0.08) had a <i>P</i> value of ≤0.2. In a covariate-adjusted model, more experienced centers were associated with a 70% lower hazard of graft failure (hazard ratio, 0.29; 95% confidence interval, 0.12-0.70; <i>P</i> = 0.006) and 72% lower hazard of mortality (hazard ratio, 0.27; confidence interval, 0.11-0.69; <i>P</i> = 0.007).</p><p><strong>Conclusions: </strong>These data suggest that experienced centers have improved posttransplant survival. Variations in selection and postoperative care not captured by this study may underlie this association. More granular studies are warranted to elucidate the impact of center experience on outcomes in transplantation for cholangiocarcinoma.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 7","pages":"e1822"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208638/pdf/","citationCount":"0","resultStr":"{\"title\":\"Center Experience Is Associated With Improved Survival in Liver Transplantation for Hilar Cholangiocarcinoma: A Retrospective Study.\",\"authors\":\"Omar Bushara, Yash Kadakia, Katharine Krupp, Jessica Friedman, Maarouf A Hoteit, Therese Bittermann, Tarek Araji, Matthew H Levine\",\"doi\":\"10.1097/TXD.0000000000001822\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hilar cholangiocarcinoma has limited treatments, with transplantation emerging as a curative option. During the era of regional patient review, it was suggested that transplant centers performing a higher volume of transplants for cholangiocarcinoma had improved outcomes. However, it is unknown whether this association persists since the national standardization of guidelines in May 2019.</p><p><strong>Methods: </strong>Transplant candidates listed in the United Network of Organ Sharing database using cholangiocarcinoma exception points from May 2019 to December 2022 were included. Experienced centers were defined as performing at least 10 transplants during the time period. Recipient and donor characteristics, graft and patient survival, and hospital length of stay were compared between more and less experienced centers. The Wilcoxon rank-sum test, Fisher exact test, Kaplan-Meier curves, log-rank tests, and Cox hazards analyses were used where appropriate.</p><p><strong>Results: </strong>Between May 2019 and December 2022, 166 transplants for cholangiocarcinoma were performed at 37 centers, with \\\"more experienced\\\" centers accounting for 59% (n = 98). Unadjusted graft survival (<i>P</i> = 0.03) and patient survival (<i>P</i> = 0.047) were lower at less experienced centers. In addition to center experience, univariable Cox analyses recipient age (0.02), diabetes (0.18), and donor age (0.08) had a <i>P</i> value of ≤0.2. In a covariate-adjusted model, more experienced centers were associated with a 70% lower hazard of graft failure (hazard ratio, 0.29; 95% confidence interval, 0.12-0.70; <i>P</i> = 0.006) and 72% lower hazard of mortality (hazard ratio, 0.27; confidence interval, 0.11-0.69; <i>P</i> = 0.007).</p><p><strong>Conclusions: </strong>These data suggest that experienced centers have improved posttransplant survival. Variations in selection and postoperative care not captured by this study may underlie this association. More granular studies are warranted to elucidate the impact of center experience on outcomes in transplantation for cholangiocarcinoma.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"11 7\",\"pages\":\"e1822\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208638/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001822\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001822","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
Center Experience Is Associated With Improved Survival in Liver Transplantation for Hilar Cholangiocarcinoma: A Retrospective Study.
Background: Hilar cholangiocarcinoma has limited treatments, with transplantation emerging as a curative option. During the era of regional patient review, it was suggested that transplant centers performing a higher volume of transplants for cholangiocarcinoma had improved outcomes. However, it is unknown whether this association persists since the national standardization of guidelines in May 2019.
Methods: Transplant candidates listed in the United Network of Organ Sharing database using cholangiocarcinoma exception points from May 2019 to December 2022 were included. Experienced centers were defined as performing at least 10 transplants during the time period. Recipient and donor characteristics, graft and patient survival, and hospital length of stay were compared between more and less experienced centers. The Wilcoxon rank-sum test, Fisher exact test, Kaplan-Meier curves, log-rank tests, and Cox hazards analyses were used where appropriate.
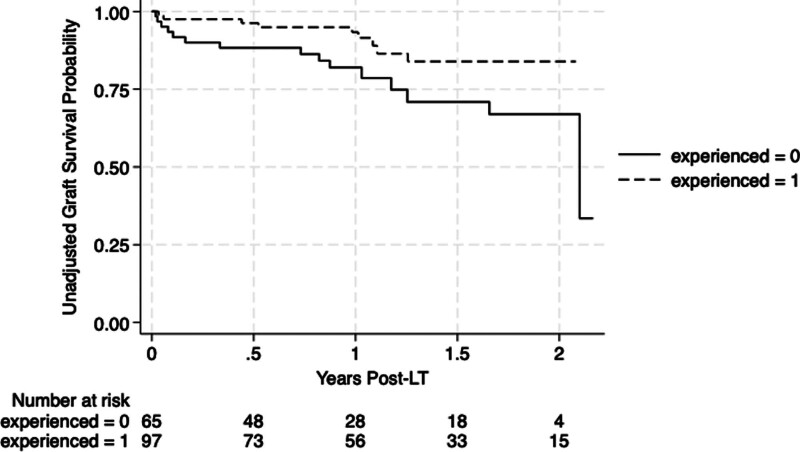
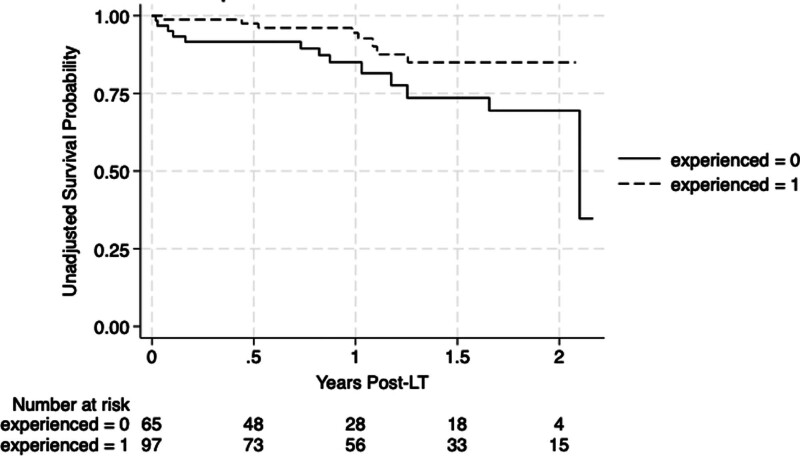
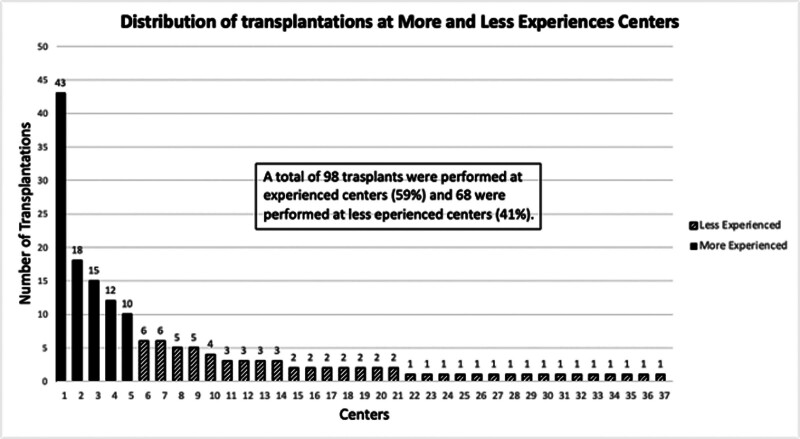
Results: Between May 2019 and December 2022, 166 transplants for cholangiocarcinoma were performed at 37 centers, with "more experienced" centers accounting for 59% (n = 98). Unadjusted graft survival (P = 0.03) and patient survival (P = 0.047) were lower at less experienced centers. In addition to center experience, univariable Cox analyses recipient age (0.02), diabetes (0.18), and donor age (0.08) had a P value of ≤0.2. In a covariate-adjusted model, more experienced centers were associated with a 70% lower hazard of graft failure (hazard ratio, 0.29; 95% confidence interval, 0.12-0.70; P = 0.006) and 72% lower hazard of mortality (hazard ratio, 0.27; confidence interval, 0.11-0.69; P = 0.007).
Conclusions: These data suggest that experienced centers have improved posttransplant survival. Variations in selection and postoperative care not captured by this study may underlie this association. More granular studies are warranted to elucidate the impact of center experience on outcomes in transplantation for cholangiocarcinoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


