Chenglong Duan, Jinsui Du, Lizhe Zhu, Man Niu, Dong Fan, Siyuan Jiang, Jiaqi Zhang, Yudong Zhou, Yi Pan, Danni Li, Jianing Zhang, Yu Ren, Bin Wang
{"title":"预测乳腺导管原位癌术后升级的DCIS-IBC指南板:来自多中心研究的临床见解。","authors":"Chenglong Duan, Jinsui Du, Lizhe Zhu, Man Niu, Dong Fan, Siyuan Jiang, Jiaqi Zhang, Yudong Zhou, Yi Pan, Danni Li, Jianing Zhang, Yu Ren, Bin Wang","doi":"10.1007/s10549-025-07763-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ductal carcinoma in situ (DCIS) carries a significant risk of postoperative upgrading to invasive breast cancer (IBC), yet existing prediction models lack validation in Asian populations. This study aimed to develop and validate a population-specific nomogram to preoperatively predict DCIS-to-IBC upgrading in Asian patients.</p><p><strong>Methods: </strong>A multicenter retrospective cohort of 465 Asian women diagnosed with DCIS by core needle biopsy (2015-2021) was analyzed. Patients were randomly divided into training (n = 257), internal validation (n = 110), and external validation cohorts (n = 98). Predictors were selected via LASSO regression and multivariable logistic regression. Model performance was assessed using AUC, calibration curves, and decision curve analysis (DCA). An interactive online nomogram was developed for clinical application.</p><p><strong>Results: </strong>Postoperative upgrading occurred in 49.46% (230/465) of patients. Four independent predictors were identified: palpable mass (OR = 2.55, p = 0.096), lesion palpability (OR = 2.58, p = 0.043), low nuclear grade (OR = 0.55, p = 0.098), and suspected invasion (OR = 6.59, p < 0.001). The nomogram demonstrated robust discrimination in the training cohort (AUC = 0.802, 95% CI 0.748-0.856), with maintained performance in internal validation (AUC = 0.753) and acceptable generalizability in external validation (AUC = 0.680). DCA confirmed clinical utility across risk thresholds. The dynamic nomogram ( https://duancl777.shinyapps.io/dynnomapp/ ) enabled real-time risk stratification.</p><p><strong>Conclusions: </strong>The DCIS-IBC Guide Board is the first Asian-specific model integrating clinicopathological predictors to identify high-risk DCIS patients. It facilitates personalized decisions, such as omitting sentinel lymph node biopsy while reducing overtreatment. Although external validation showed moderate performance, this tool addresses critical population heterogeneity and enhances preoperative risk assessment. Prospective multicenter studies are warranted to optimize generalizability and explore multimodal predictors.</p>","PeriodicalId":9133,"journal":{"name":"Breast Cancer Research and Treatment","volume":" ","pages":"101-114"},"PeriodicalIF":3.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12259714/pdf/","citationCount":"0","resultStr":"{\"title\":\"The DCIS-IBC guide board on predicting postoperative upgrading in breast ductal carcinoma in situ: clinical insights from a multicenter study.\",\"authors\":\"Chenglong Duan, Jinsui Du, Lizhe Zhu, Man Niu, Dong Fan, Siyuan Jiang, Jiaqi Zhang, Yudong Zhou, Yi Pan, Danni Li, Jianing Zhang, Yu Ren, Bin Wang\",\"doi\":\"10.1007/s10549-025-07763-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ductal carcinoma in situ (DCIS) carries a significant risk of postoperative upgrading to invasive breast cancer (IBC), yet existing prediction models lack validation in Asian populations. This study aimed to develop and validate a population-specific nomogram to preoperatively predict DCIS-to-IBC upgrading in Asian patients.</p><p><strong>Methods: </strong>A multicenter retrospective cohort of 465 Asian women diagnosed with DCIS by core needle biopsy (2015-2021) was analyzed. Patients were randomly divided into training (n = 257), internal validation (n = 110), and external validation cohorts (n = 98). Predictors were selected via LASSO regression and multivariable logistic regression. Model performance was assessed using AUC, calibration curves, and decision curve analysis (DCA). An interactive online nomogram was developed for clinical application.</p><p><strong>Results: </strong>Postoperative upgrading occurred in 49.46% (230/465) of patients. Four independent predictors were identified: palpable mass (OR = 2.55, p = 0.096), lesion palpability (OR = 2.58, p = 0.043), low nuclear grade (OR = 0.55, p = 0.098), and suspected invasion (OR = 6.59, p < 0.001). The nomogram demonstrated robust discrimination in the training cohort (AUC = 0.802, 95% CI 0.748-0.856), with maintained performance in internal validation (AUC = 0.753) and acceptable generalizability in external validation (AUC = 0.680). DCA confirmed clinical utility across risk thresholds. The dynamic nomogram ( https://duancl777.shinyapps.io/dynnomapp/ ) enabled real-time risk stratification.</p><p><strong>Conclusions: </strong>The DCIS-IBC Guide Board is the first Asian-specific model integrating clinicopathological predictors to identify high-risk DCIS patients. It facilitates personalized decisions, such as omitting sentinel lymph node biopsy while reducing overtreatment. Although external validation showed moderate performance, this tool addresses critical population heterogeneity and enhances preoperative risk assessment. Prospective multicenter studies are warranted to optimize generalizability and explore multimodal predictors.</p>\",\"PeriodicalId\":9133,\"journal\":{\"name\":\"Breast Cancer Research and Treatment\",\"volume\":\" \",\"pages\":\"101-114\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12259714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Breast Cancer Research and Treatment\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10549-025-07763-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer Research and Treatment","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10549-025-07763-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:导管原位癌(DCIS)具有显著的术后升级为浸润性乳腺癌(IBC)的风险,但现有的预测模型在亚洲人群中缺乏验证。本研究旨在开发和验证一种人群特异性nomogram,用于预测亚洲患者术前dcis到ibc的升级。方法:对2015-2021年465名经核心针活检诊断为DCIS的亚洲女性进行多中心回顾性队列分析。患者被随机分为训练组(n = 257)、内部验证组(n = 110)和外部验证组(n = 98)。通过LASSO回归和多变量logistic回归选择预测因子。采用AUC、校准曲线和决策曲线分析(DCA)评估模型性能。为临床应用开发了一种互动式在线心电图。结果:术后升级率为49.46%(230/465)。发现了四个独立的预测因素:可触及的肿块(OR = 2.55, p = 0.096)、病变可触及性(OR = 2.58, p = 0.043)、低核分级(OR = 0.55, p = 0.098)和疑似侵袭(OR = 6.59, p)。结论:DCIS- ibc指南委员会是第一个整合临床病理预测因素来识别高危DCIS患者的亚洲特异性模型。它有助于个性化的决定,如省略前哨淋巴结活检,同时减少过度治疗。虽然外部验证显示表现一般,但该工具解决了关键的人群异质性并增强了术前风险评估。有必要进行前瞻性多中心研究,以优化通用性并探索多模态预测因子。
The DCIS-IBC guide board on predicting postoperative upgrading in breast ductal carcinoma in situ: clinical insights from a multicenter study.
Background: Ductal carcinoma in situ (DCIS) carries a significant risk of postoperative upgrading to invasive breast cancer (IBC), yet existing prediction models lack validation in Asian populations. This study aimed to develop and validate a population-specific nomogram to preoperatively predict DCIS-to-IBC upgrading in Asian patients.
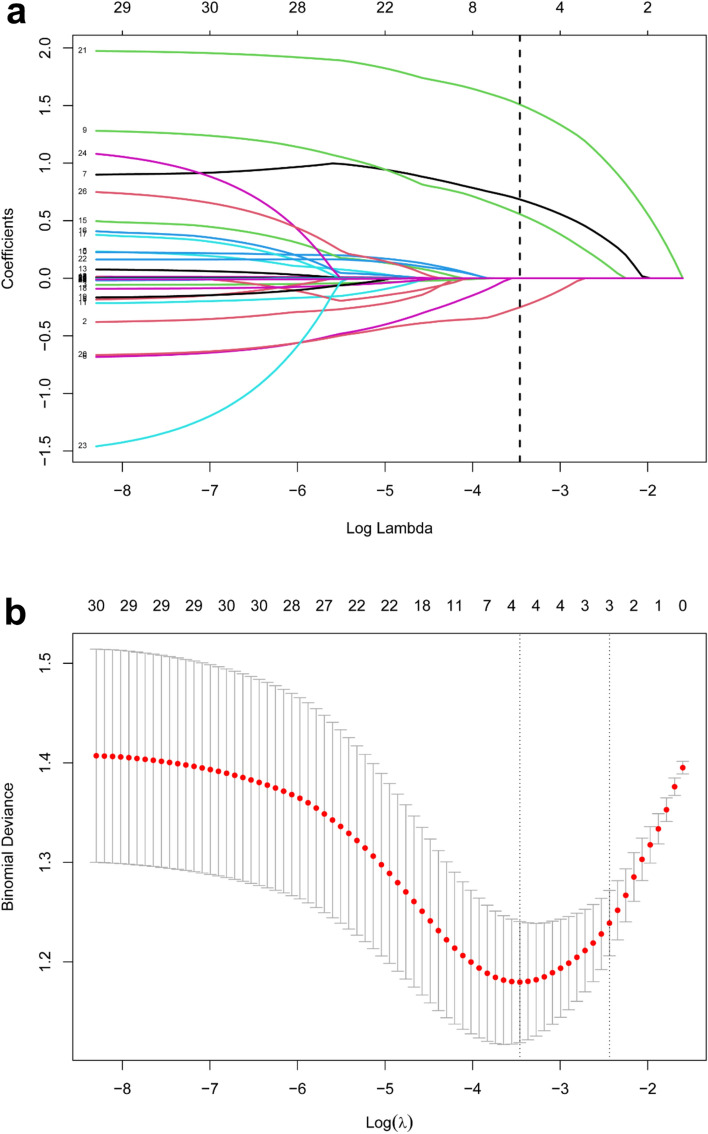
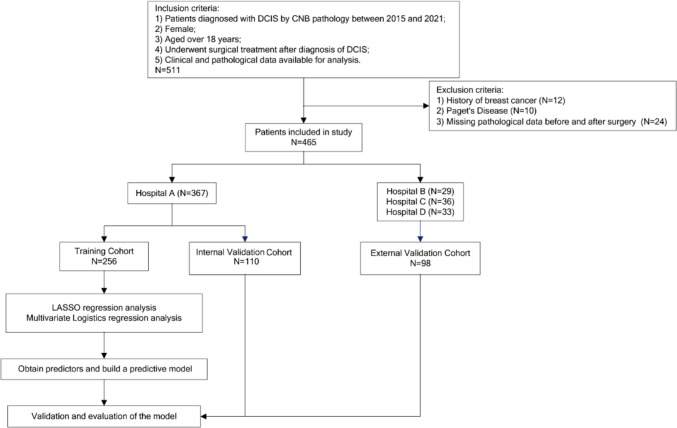
Methods: A multicenter retrospective cohort of 465 Asian women diagnosed with DCIS by core needle biopsy (2015-2021) was analyzed. Patients were randomly divided into training (n = 257), internal validation (n = 110), and external validation cohorts (n = 98). Predictors were selected via LASSO regression and multivariable logistic regression. Model performance was assessed using AUC, calibration curves, and decision curve analysis (DCA). An interactive online nomogram was developed for clinical application.
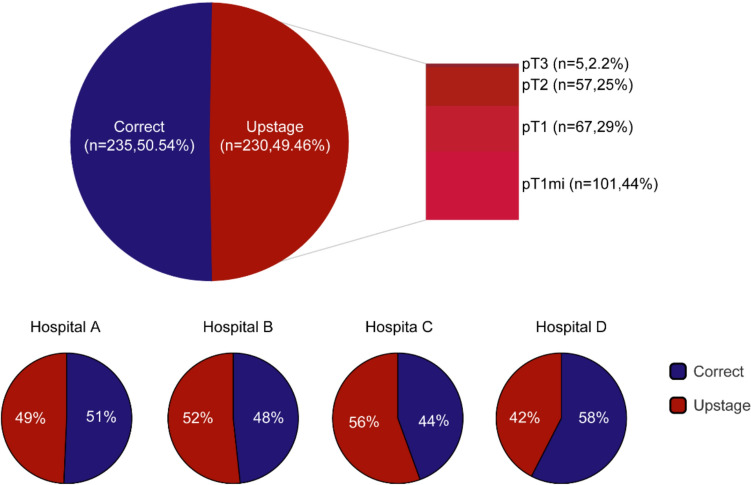
Results: Postoperative upgrading occurred in 49.46% (230/465) of patients. Four independent predictors were identified: palpable mass (OR = 2.55, p = 0.096), lesion palpability (OR = 2.58, p = 0.043), low nuclear grade (OR = 0.55, p = 0.098), and suspected invasion (OR = 6.59, p < 0.001). The nomogram demonstrated robust discrimination in the training cohort (AUC = 0.802, 95% CI 0.748-0.856), with maintained performance in internal validation (AUC = 0.753) and acceptable generalizability in external validation (AUC = 0.680). DCA confirmed clinical utility across risk thresholds. The dynamic nomogram ( https://duancl777.shinyapps.io/dynnomapp/ ) enabled real-time risk stratification.
Conclusions: The DCIS-IBC Guide Board is the first Asian-specific model integrating clinicopathological predictors to identify high-risk DCIS patients. It facilitates personalized decisions, such as omitting sentinel lymph node biopsy while reducing overtreatment. Although external validation showed moderate performance, this tool addresses critical population heterogeneity and enhances preoperative risk assessment. Prospective multicenter studies are warranted to optimize generalizability and explore multimodal predictors.
期刊介绍:
Breast Cancer Research and Treatment provides the surgeon, radiotherapist, medical oncologist, endocrinologist, epidemiologist, immunologist or cell biologist investigating problems in breast cancer a single forum for communication. The journal creates a "market place" for breast cancer topics which cuts across all the usual lines of disciplines, providing a site for presenting pertinent investigations, and for discussing critical questions relevant to the entire field. It seeks to develop a new focus and new perspectives for all those concerned with breast cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


