{"title":"附加经验性上腔静脉隔离对病态窦房综合征房颤患者窦结功能的中期影响","authors":"Miwa Kanai MD, PhD, Satoshi Higuchi MD, PhD, Masayuki Sakai MD, Yuko Matsui MD, Shun Hasegawa MD, Daigo Yagishita MD, PhD, Morio Shoda MD, PhD, Junichi Yamaguchi MD, PhD","doi":"10.1002/joa3.70126","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>The safety of including superior vena cava isolation (SVCI) along with pulmonary vein isolation (PVI) in atrial fibrillation (AF) patients with sick sinus syndrome (SSS) remains uncertain, as this decision is often left to the discretion of individual physicians.</p>\n </section>\n \n <section>\n \n <h3> Methods and Results</h3>\n \n <p>In this retrospective study, 94 AF patients with SSS, who underwent PVI without prior pacemaker placement, were divided into two groups: those with (<i>n</i> = 67, age 66.0 ± 9.3 years, male 61%) and without (<i>n</i> = 27, age 66.6 ± 10.0 years, male 63%) additional empirical SVCI. SVCI was performed at 25–35 W, 10–20 mm superior to the earliest sites of activation during sinus rhythm. The primary endpoint compared atrial tachyarrhythmia (ATA) recurrence, pacemaker avoidance, and 24-hour ambulatory monitoring results between the SVCI and non-SVCI groups. Preprocedure minimum heart rate (SVCI 37.6 ± 11.6 Bpm vs. non-SVCI 37.0 ± 9.9 Bpm, <i>p</i> = 0.74) and maximum pause (SVCI 4.2 ± 2.7 Sec vs. non-SVCI 3.6 ± 2.8 Sec, <i>p</i> = 0.15) were not different between the two groups. During 36 months of follow-up after the last procedure, ATA recurrence rates (SVCI 33% vs. non-SVCI 34%, <i>p</i> = 0.82) and pacemaker avoidance rates (SVCI 84% vs. non-SVCI 93%, <i>p</i> = 0.32) Were Comparable between the two groups. At 36 months after the last procedure, minimum heart rate (SVCI 48.7 ± 10.2 bpm vs. non-SVCI 47.4 ± 8.3 bpm, <i>p</i> = 0.52) and maximum pause (SVCI 1.6 ± 1.0 sec vs. non-SVCI 1.6 ± 0.6 sec, <i>p</i> = 0.33) remained similar between the two groups.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In this study, the addition of SVCI did not significantly increase the need for pacemaker implantation or lead to sinus node dysfunction in AF patients with SSS compared to PVI alone.</p>\n </section>\n </div>","PeriodicalId":15174,"journal":{"name":"Journal of Arrhythmia","volume":"41 4","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/joa3.70126","citationCount":"0","resultStr":"{\"title\":\"Mid-term effects on sinus node function following additional empirical superior vena cava isolation in atrial fibrillation patients with sick sinus syndrome\",\"authors\":\"Miwa Kanai MD, PhD, Satoshi Higuchi MD, PhD, Masayuki Sakai MD, Yuko Matsui MD, Shun Hasegawa MD, Daigo Yagishita MD, PhD, Morio Shoda MD, PhD, Junichi Yamaguchi MD, PhD\",\"doi\":\"10.1002/joa3.70126\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>The safety of including superior vena cava isolation (SVCI) along with pulmonary vein isolation (PVI) in atrial fibrillation (AF) patients with sick sinus syndrome (SSS) remains uncertain, as this decision is often left to the discretion of individual physicians.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and Results</h3>\\n \\n <p>In this retrospective study, 94 AF patients with SSS, who underwent PVI without prior pacemaker placement, were divided into two groups: those with (<i>n</i> = 67, age 66.0 ± 9.3 years, male 61%) and without (<i>n</i> = 27, age 66.6 ± 10.0 years, male 63%) additional empirical SVCI. SVCI was performed at 25–35 W, 10–20 mm superior to the earliest sites of activation during sinus rhythm. The primary endpoint compared atrial tachyarrhythmia (ATA) recurrence, pacemaker avoidance, and 24-hour ambulatory monitoring results between the SVCI and non-SVCI groups. Preprocedure minimum heart rate (SVCI 37.6 ± 11.6 Bpm vs. non-SVCI 37.0 ± 9.9 Bpm, <i>p</i> = 0.74) and maximum pause (SVCI 4.2 ± 2.7 Sec vs. non-SVCI 3.6 ± 2.8 Sec, <i>p</i> = 0.15) were not different between the two groups. During 36 months of follow-up after the last procedure, ATA recurrence rates (SVCI 33% vs. non-SVCI 34%, <i>p</i> = 0.82) and pacemaker avoidance rates (SVCI 84% vs. non-SVCI 93%, <i>p</i> = 0.32) Were Comparable between the two groups. At 36 months after the last procedure, minimum heart rate (SVCI 48.7 ± 10.2 bpm vs. non-SVCI 47.4 ± 8.3 bpm, <i>p</i> = 0.52) and maximum pause (SVCI 1.6 ± 1.0 sec vs. non-SVCI 1.6 ± 0.6 sec, <i>p</i> = 0.33) remained similar between the two groups.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In this study, the addition of SVCI did not significantly increase the need for pacemaker implantation or lead to sinus node dysfunction in AF patients with SSS compared to PVI alone.</p>\\n </section>\\n </div>\",\"PeriodicalId\":15174,\"journal\":{\"name\":\"Journal of Arrhythmia\",\"volume\":\"41 4\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/joa3.70126\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Arrhythmia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/joa3.70126\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Arrhythmia","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/joa3.70126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Mid-term effects on sinus node function following additional empirical superior vena cava isolation in atrial fibrillation patients with sick sinus syndrome
Aim
The safety of including superior vena cava isolation (SVCI) along with pulmonary vein isolation (PVI) in atrial fibrillation (AF) patients with sick sinus syndrome (SSS) remains uncertain, as this decision is often left to the discretion of individual physicians.
Methods and Results
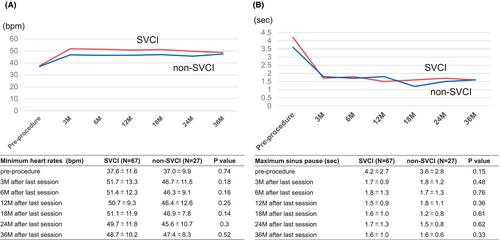
In this retrospective study, 94 AF patients with SSS, who underwent PVI without prior pacemaker placement, were divided into two groups: those with (n = 67, age 66.0 ± 9.3 years, male 61%) and without (n = 27, age 66.6 ± 10.0 years, male 63%) additional empirical SVCI. SVCI was performed at 25–35 W, 10–20 mm superior to the earliest sites of activation during sinus rhythm. The primary endpoint compared atrial tachyarrhythmia (ATA) recurrence, pacemaker avoidance, and 24-hour ambulatory monitoring results between the SVCI and non-SVCI groups. Preprocedure minimum heart rate (SVCI 37.6 ± 11.6 Bpm vs. non-SVCI 37.0 ± 9.9 Bpm, p = 0.74) and maximum pause (SVCI 4.2 ± 2.7 Sec vs. non-SVCI 3.6 ± 2.8 Sec, p = 0.15) were not different between the two groups. During 36 months of follow-up after the last procedure, ATA recurrence rates (SVCI 33% vs. non-SVCI 34%, p = 0.82) and pacemaker avoidance rates (SVCI 84% vs. non-SVCI 93%, p = 0.32) Were Comparable between the two groups. At 36 months after the last procedure, minimum heart rate (SVCI 48.7 ± 10.2 bpm vs. non-SVCI 47.4 ± 8.3 bpm, p = 0.52) and maximum pause (SVCI 1.6 ± 1.0 sec vs. non-SVCI 1.6 ± 0.6 sec, p = 0.33) remained similar between the two groups.
Conclusion
In this study, the addition of SVCI did not significantly increase the need for pacemaker implantation or lead to sinus node dysfunction in AF patients with SSS compared to PVI alone.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


