Julius Jelisejevas, Ali Husain, Brian Chiang, Sophie Offen, Gnalini Sathananthan, Robert Moss, Jonathon A Leipsic, Philipp Blanke, Janarthanan Sathananthan, Robert H Boone, John G Webb, David A Wood, Anson Cheung
{"title":"三尖瓣反流的晚期转诊和高死亡率:呼吁及时干预。","authors":"Julius Jelisejevas, Ali Husain, Brian Chiang, Sophie Offen, Gnalini Sathananthan, Robert Moss, Jonathon A Leipsic, Philipp Blanke, Janarthanan Sathananthan, Robert H Boone, John G Webb, David A Wood, Anson Cheung","doi":"10.1093/ehjopen/oeaf072","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Tricuspid regurgitation (TR) is associated with increased morbidity and mortality. The optimal timing for referral and intervention remains uncertain. To evaluate outcomes in patients with TR referred for tricuspid valve intervention.</p><p><strong>Methods and results: </strong>Fifty-eight consecutive patients were referred from May 2018 to April 2023. Patients were stratified into two groups: Group 1 who underwent either tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve replacement (TTVR); Group 2 who died without intervention due to: awaiting candidacy assessment; awaiting intervention; deemed unsuitable for intervention. Key endpoints: in-patient, 30-day, 12- and 18-month mortality; new pacemaker implantation; echocardiographic TR grading; improvement in NYHA functional class; and heart failure-related readmissions at 30 days and 12 months. Among 58 patients, 43 underwent intervention (TTVR, <i>n</i> = 29; T-TEER, <i>n</i> = 14), 15 died without intervention (awaiting assessment <i>n</i> = 11; awaiting procedure <i>n</i> = 1, unsuitable <i>n</i> = 3). At the time of referral, the mean age was 77.0 ± 9.8 years, and 52 patients (90%) were diagnosed with functional TR; 30-day mortality in Group 1 was 12%, and 12-month mortality reached 33%, with heart failure readmission (37%); 12-month mortality in Group 2 was 73%. At 18 months, mortality reached 37% in Group 1 and 100% in Group 2. Baseline characteristics differed significantly between the groups for body mass index, severity of TR (massive or torrential), NYHA III-IV symptoms, and validated mortality scores.</p><p><strong>Conclusion: </strong>Referrals for TR often occur after substantial comorbidities have developed resulting in high mortality but should be considered for a referral and intervention at an earlier stage.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf072"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12198771/pdf/","citationCount":"0","resultStr":"{\"title\":\"Late referrals and high mortality in tricuspid regurgitation: a call for timely intervention.\",\"authors\":\"Julius Jelisejevas, Ali Husain, Brian Chiang, Sophie Offen, Gnalini Sathananthan, Robert Moss, Jonathon A Leipsic, Philipp Blanke, Janarthanan Sathananthan, Robert H Boone, John G Webb, David A Wood, Anson Cheung\",\"doi\":\"10.1093/ehjopen/oeaf072\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Tricuspid regurgitation (TR) is associated with increased morbidity and mortality. The optimal timing for referral and intervention remains uncertain. To evaluate outcomes in patients with TR referred for tricuspid valve intervention.</p><p><strong>Methods and results: </strong>Fifty-eight consecutive patients were referred from May 2018 to April 2023. Patients were stratified into two groups: Group 1 who underwent either tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve replacement (TTVR); Group 2 who died without intervention due to: awaiting candidacy assessment; awaiting intervention; deemed unsuitable for intervention. Key endpoints: in-patient, 30-day, 12- and 18-month mortality; new pacemaker implantation; echocardiographic TR grading; improvement in NYHA functional class; and heart failure-related readmissions at 30 days and 12 months. Among 58 patients, 43 underwent intervention (TTVR, <i>n</i> = 29; T-TEER, <i>n</i> = 14), 15 died without intervention (awaiting assessment <i>n</i> = 11; awaiting procedure <i>n</i> = 1, unsuitable <i>n</i> = 3). At the time of referral, the mean age was 77.0 ± 9.8 years, and 52 patients (90%) were diagnosed with functional TR; 30-day mortality in Group 1 was 12%, and 12-month mortality reached 33%, with heart failure readmission (37%); 12-month mortality in Group 2 was 73%. At 18 months, mortality reached 37% in Group 1 and 100% in Group 2. Baseline characteristics differed significantly between the groups for body mass index, severity of TR (massive or torrential), NYHA III-IV symptoms, and validated mortality scores.</p><p><strong>Conclusion: </strong>Referrals for TR often occur after substantial comorbidities have developed resulting in high mortality but should be considered for a referral and intervention at an earlier stage.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf072\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12198771/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf072\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:三尖瓣反流(TR)与发病率和死亡率增加有关。转诊和干预的最佳时机仍不确定。评价TR患者行三尖瓣介入治疗的结果。方法与结果:2018年5月至2023年4月,连续转介58例患者。患者被分为两组:1组接受三尖瓣经导管边缘到边缘修复(T-TEER)或经导管三尖瓣置换术(TTVR);第2组未干预死亡,原因如下:等待候选资格评估;等待干预;认为不适合干预的。关键终点:住院、30天、12个月和18个月死亡率;新型起搏器植入;超声心动图TR分级;NYHA功能分级改善;30天和12个月心力衰竭相关的再入院。58例患者中,43例接受了干预(TTVR, n = 29;T-TEER, n = 14),未经干预死亡15例(等待评估n = 11;等待程序n = 1,不适合程序n = 3)。转诊时平均年龄为77.0±9.8岁,52例(90%)诊断为功能性TR;第1组30天死亡率为12%,12个月死亡率为33%,心力衰竭再入院(37%);第2组12个月死亡率为73%。18个月时,第1组死亡率为37%,第2组为100%。各组之间的基线特征在体重指数、TR严重程度(严重或严重)、NYHA III-IV症状和验证死亡率评分方面存在显著差异。结论:TR的转诊通常发生在大量合并症发展导致高死亡率之后,但应考虑在早期阶段进行转诊和干预。
Late referrals and high mortality in tricuspid regurgitation: a call for timely intervention.
Aims: Tricuspid regurgitation (TR) is associated with increased morbidity and mortality. The optimal timing for referral and intervention remains uncertain. To evaluate outcomes in patients with TR referred for tricuspid valve intervention.
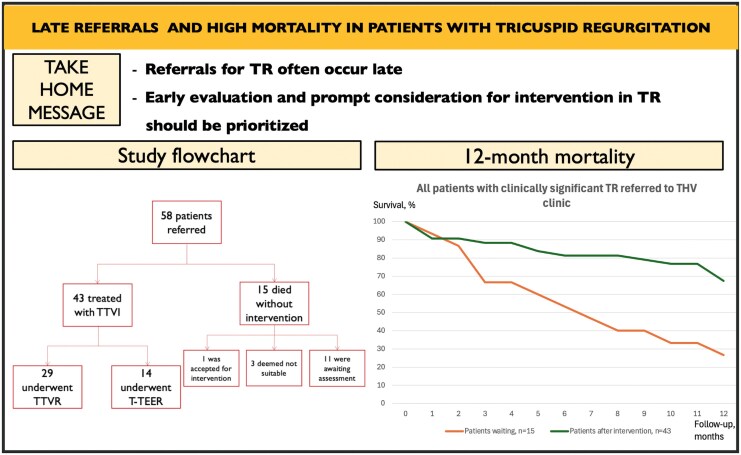
Methods and results: Fifty-eight consecutive patients were referred from May 2018 to April 2023. Patients were stratified into two groups: Group 1 who underwent either tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve replacement (TTVR); Group 2 who died without intervention due to: awaiting candidacy assessment; awaiting intervention; deemed unsuitable for intervention. Key endpoints: in-patient, 30-day, 12- and 18-month mortality; new pacemaker implantation; echocardiographic TR grading; improvement in NYHA functional class; and heart failure-related readmissions at 30 days and 12 months. Among 58 patients, 43 underwent intervention (TTVR, n = 29; T-TEER, n = 14), 15 died without intervention (awaiting assessment n = 11; awaiting procedure n = 1, unsuitable n = 3). At the time of referral, the mean age was 77.0 ± 9.8 years, and 52 patients (90%) were diagnosed with functional TR; 30-day mortality in Group 1 was 12%, and 12-month mortality reached 33%, with heart failure readmission (37%); 12-month mortality in Group 2 was 73%. At 18 months, mortality reached 37% in Group 1 and 100% in Group 2. Baseline characteristics differed significantly between the groups for body mass index, severity of TR (massive or torrential), NYHA III-IV symptoms, and validated mortality scores.
Conclusion: Referrals for TR often occur after substantial comorbidities have developed resulting in high mortality but should be considered for a referral and intervention at an earlier stage.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


