Sérgio R R Decker, Danielle do A Pereira, Gabriela S Rech, Rosa da R M Dos Santos, Denise de Souza, Raíne F De Carli, Geraldine Trott, Ana P de Souza, Janine Gonzaga, Lauren S Costa, Jonas M Wolf, Gregory S Medeiros, Bruna Conte, Laura C Madeira, Livia Biason, Maria D Rosa, Mariana F Mattioni, Isabela T Muller, Carolia Bayer, Odanor F T Filho, Marcelo Kern, Cassiano Teixeira, Harris L Carmichael, Victor D Dinglas, Samuel M Brown, Dale M Needham, Regis G Rosa
{"title":"巴西急性呼吸衰竭幸存者出院后未满足的非药物治疗需求和不良后果:一项前瞻性可行性研究","authors":"Sérgio R R Decker, Danielle do A Pereira, Gabriela S Rech, Rosa da R M Dos Santos, Denise de Souza, Raíne F De Carli, Geraldine Trott, Ana P de Souza, Janine Gonzaga, Lauren S Costa, Jonas M Wolf, Gregory S Medeiros, Bruna Conte, Laura C Madeira, Livia Biason, Maria D Rosa, Mariana F Mattioni, Isabela T Muller, Carolia Bayer, Odanor F T Filho, Marcelo Kern, Cassiano Teixeira, Harris L Carmichael, Victor D Dinglas, Samuel M Brown, Dale M Needham, Regis G Rosa","doi":"10.1097/CCE.0000000000001279","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>In-hospital survivorship for acute respiratory failure has improved, but unmet nonmedication healthcare needs may contribute to adverse events post-discharge.</p><p><strong>Objectives: </strong>To evaluate the feasibility of characterizing early unmet nonmedication discharge needs, classified as durable medical equipment (DME), home health services (HHS), and follow-up medical appointments (FUA) for acute respiratory failure survivors in Brazil. Secondary objectives include describing the profile of needs, unmet needs, and adverse outcomes post-discharge.</p><p><strong>Design: </strong>Prospective feasibility cohort study, with enrollment between October 2020 and March 2021.</p><p><strong>Setting: </strong>One tertiary teaching hospital from Southern Brazil with 76 ICU beds.</p><p><strong>Participants: </strong>Adult survivors from acute respiratory failure who were discharged home.</p><p><strong>Main outcomes and measures: </strong>Our primary outcome was the feasibility of measuring unmet nonmedication needs between 7 and 28 days post-discharge, considering greater than 80% of data completeness as feasible. Secondary outcomes included the characterization of needs and needs unmet per type at 1 month and the crude risk of all-cause death, hospital readmission, and urgent visits to the emergency department at 3 months post-discharge.</p><p><strong>Results: </strong>Of 337 patients screened, 72 were enrolled, and data on unmet nonmedication needs were collected from 66 patients, resulting in a primary feasibility outcome of 91.7%. The median age was 59 years, 38.9% were female, most were self-declared White, and were employed before admission. During the index admission, 87.3% were diagnosed with COVID-19, and 79.2% received invasive mechanical ventilation. The frequency of nonmedication discharge needs was 48 (72.7%) for DME, 54 (81.8%) for HHS, and 60 (90.9%) for FUA. At 1 month, 36 (58.1%) had at least one need unmet; at 3 months, 12 (19.0%) had at least one adverse outcome.</p><p><strong>Conclusions and relevance: </strong>Detailed measurement of nonmedication needs post-discharge for acute respiratory failure survivors in Brazil is feasible. Unmet nonmedication needs are a common problem to be addressed in this population.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 7","pages":"e1279"},"PeriodicalIF":2.7000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245325/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unmet Nonmedication Needs After Hospital Discharge and Adverse Outcomes Among Acute Respiratory Failure Survivors in Brazil: A Prospective Feasibility Study.\",\"authors\":\"Sérgio R R Decker, Danielle do A Pereira, Gabriela S Rech, Rosa da R M Dos Santos, Denise de Souza, Raíne F De Carli, Geraldine Trott, Ana P de Souza, Janine Gonzaga, Lauren S Costa, Jonas M Wolf, Gregory S Medeiros, Bruna Conte, Laura C Madeira, Livia Biason, Maria D Rosa, Mariana F Mattioni, Isabela T Muller, Carolia Bayer, Odanor F T Filho, Marcelo Kern, Cassiano Teixeira, Harris L Carmichael, Victor D Dinglas, Samuel M Brown, Dale M Needham, Regis G Rosa\",\"doi\":\"10.1097/CCE.0000000000001279\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>In-hospital survivorship for acute respiratory failure has improved, but unmet nonmedication healthcare needs may contribute to adverse events post-discharge.</p><p><strong>Objectives: </strong>To evaluate the feasibility of characterizing early unmet nonmedication discharge needs, classified as durable medical equipment (DME), home health services (HHS), and follow-up medical appointments (FUA) for acute respiratory failure survivors in Brazil. Secondary objectives include describing the profile of needs, unmet needs, and adverse outcomes post-discharge.</p><p><strong>Design: </strong>Prospective feasibility cohort study, with enrollment between October 2020 and March 2021.</p><p><strong>Setting: </strong>One tertiary teaching hospital from Southern Brazil with 76 ICU beds.</p><p><strong>Participants: </strong>Adult survivors from acute respiratory failure who were discharged home.</p><p><strong>Main outcomes and measures: </strong>Our primary outcome was the feasibility of measuring unmet nonmedication needs between 7 and 28 days post-discharge, considering greater than 80% of data completeness as feasible. Secondary outcomes included the characterization of needs and needs unmet per type at 1 month and the crude risk of all-cause death, hospital readmission, and urgent visits to the emergency department at 3 months post-discharge.</p><p><strong>Results: </strong>Of 337 patients screened, 72 were enrolled, and data on unmet nonmedication needs were collected from 66 patients, resulting in a primary feasibility outcome of 91.7%. The median age was 59 years, 38.9% were female, most were self-declared White, and were employed before admission. During the index admission, 87.3% were diagnosed with COVID-19, and 79.2% received invasive mechanical ventilation. The frequency of nonmedication discharge needs was 48 (72.7%) for DME, 54 (81.8%) for HHS, and 60 (90.9%) for FUA. At 1 month, 36 (58.1%) had at least one need unmet; at 3 months, 12 (19.0%) had at least one adverse outcome.</p><p><strong>Conclusions and relevance: </strong>Detailed measurement of nonmedication needs post-discharge for acute respiratory failure survivors in Brazil is feasible. Unmet nonmedication needs are a common problem to be addressed in this population.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 7\",\"pages\":\"e1279\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-06-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245325/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001279\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Unmet Nonmedication Needs After Hospital Discharge and Adverse Outcomes Among Acute Respiratory Failure Survivors in Brazil: A Prospective Feasibility Study.
Importance: In-hospital survivorship for acute respiratory failure has improved, but unmet nonmedication healthcare needs may contribute to adverse events post-discharge.
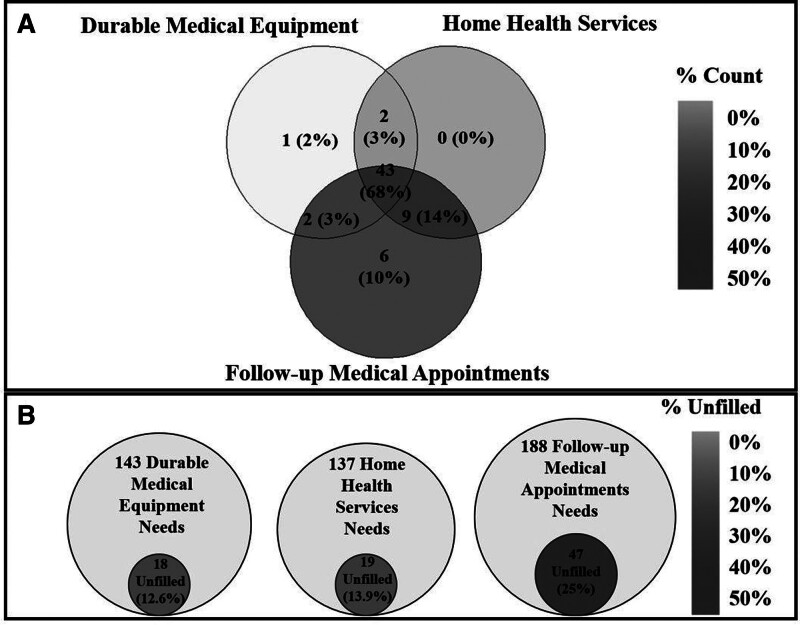
Objectives: To evaluate the feasibility of characterizing early unmet nonmedication discharge needs, classified as durable medical equipment (DME), home health services (HHS), and follow-up medical appointments (FUA) for acute respiratory failure survivors in Brazil. Secondary objectives include describing the profile of needs, unmet needs, and adverse outcomes post-discharge.
Design: Prospective feasibility cohort study, with enrollment between October 2020 and March 2021.
Setting: One tertiary teaching hospital from Southern Brazil with 76 ICU beds.
Participants: Adult survivors from acute respiratory failure who were discharged home.
Main outcomes and measures: Our primary outcome was the feasibility of measuring unmet nonmedication needs between 7 and 28 days post-discharge, considering greater than 80% of data completeness as feasible. Secondary outcomes included the characterization of needs and needs unmet per type at 1 month and the crude risk of all-cause death, hospital readmission, and urgent visits to the emergency department at 3 months post-discharge.
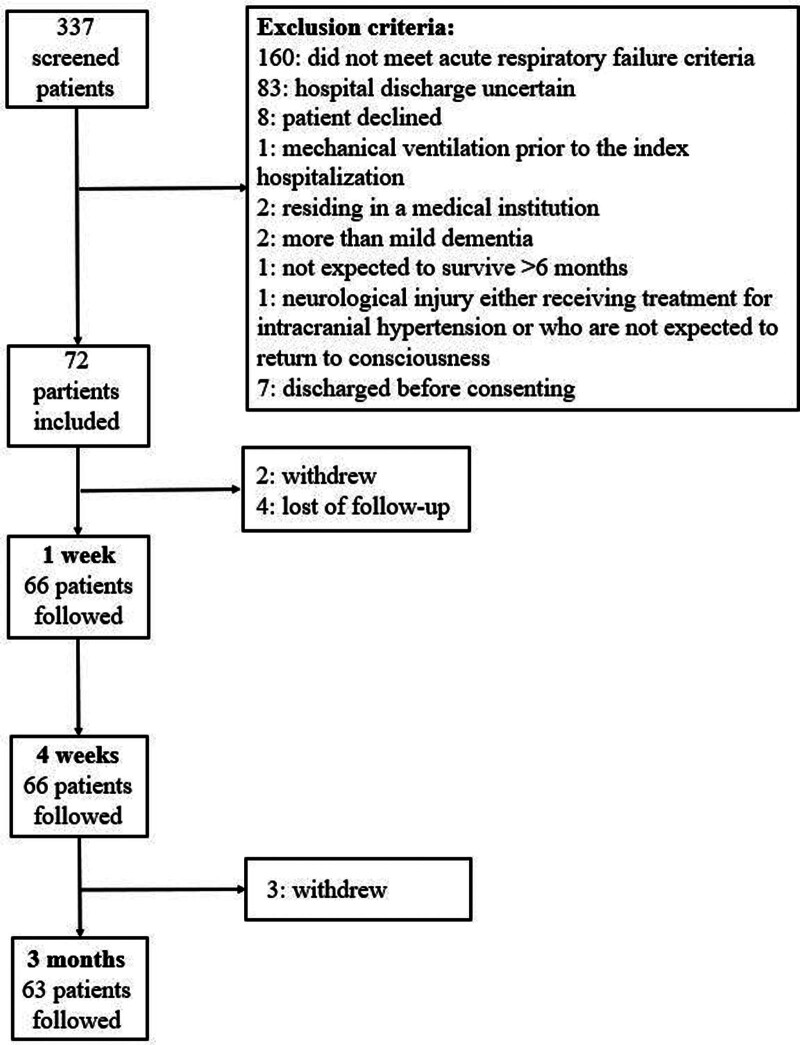
Results: Of 337 patients screened, 72 were enrolled, and data on unmet nonmedication needs were collected from 66 patients, resulting in a primary feasibility outcome of 91.7%. The median age was 59 years, 38.9% were female, most were self-declared White, and were employed before admission. During the index admission, 87.3% were diagnosed with COVID-19, and 79.2% received invasive mechanical ventilation. The frequency of nonmedication discharge needs was 48 (72.7%) for DME, 54 (81.8%) for HHS, and 60 (90.9%) for FUA. At 1 month, 36 (58.1%) had at least one need unmet; at 3 months, 12 (19.0%) had at least one adverse outcome.
Conclusions and relevance: Detailed measurement of nonmedication needs post-discharge for acute respiratory failure survivors in Brazil is feasible. Unmet nonmedication needs are a common problem to be addressed in this population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


