Kianna Cadogan, Ruth Ann Marrie, Lesley A Graff, Renee El Gabalawy, Murray W Enns, James M Bolton, Jitender Sareen, Charles N Bernstein
{"title":"炎症性肠病患者的精神共病谱","authors":"Kianna Cadogan, Ruth Ann Marrie, Lesley A Graff, Renee El Gabalawy, Murray W Enns, James M Bolton, Jitender Sareen, Charles N Bernstein","doi":"10.1093/crocol/otaf035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Research on psychiatric comorbidity in inflammatory bowel disease (IBD) has focused mostly on anxiety and depression. This study aimed to describe the spectrum of psychiatric disorders experienced by individuals with IBD and their overlap.</p><p><strong>Methods: </strong>Participants were enrolled in a prospective 3-year longitudinal study that assessed psychiatric comorbidity in immune-mediated inflammatory disease. Lifetime prevalence of psychiatric comorbidity was assessed using the Structured Clinical Interview for DSM-IV Disorders (SCID-IV), as the DSM-IV was the prevailing classification at the time of study design. Diagnosis was aligned with DSM-5 categorization where possible with available data. Psychiatric burden was categorized as no psychiatric conditions, 1, 2 or 3 or more psychiatric conditions.</p><p><strong>Results: </strong>Of 154 IBD participants (62%female, 63% Crohn's disease) 57% had at least one psychiatric comorbidity with 27% having >1 psychiatric diagnosis. The prevalence was major depressive disorder (MDD, 41.7%), anxiety disorders (39.6%; grouped as per DSM-5), substance use disorder (SUD, 16.2%), posttraumatic stress disorder (5.3%), obsessive-compulsive disorder (4.9%), and bipolar disorder (2.0%). Of participants with MDD and a comorbid psychiatric disorder, nearly half had SUD. Of those with >1 psychiatric disorder >70% had MDD and a comorbid anxiety disorder. Persons with ≥1 psychiatric comorbidity were more likely to be current smokers (<i>P</i> < .001) and to have higher IBD disease activity scores (<i>P</i> = .005) than those without a psychiatric comorbidity.</p><p><strong>Conclusions: </strong>Over half of adults with IBD had >1 diagnosed psychiatric comorbidity from a range of 10 different psychiatric disorders identified. Further research should assess the temporal relationship of IBD and the various psychiatric presentations to better understand the trajectory of co-occurrence, and therapy which may concurrently address the psychiatric disorder and the IBD.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 2","pages":"otaf035"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202087/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Spectrum of Psychiatric Comorbidity in Individuals With Inflammatory Bowel Disease.\",\"authors\":\"Kianna Cadogan, Ruth Ann Marrie, Lesley A Graff, Renee El Gabalawy, Murray W Enns, James M Bolton, Jitender Sareen, Charles N Bernstein\",\"doi\":\"10.1093/crocol/otaf035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Research on psychiatric comorbidity in inflammatory bowel disease (IBD) has focused mostly on anxiety and depression. This study aimed to describe the spectrum of psychiatric disorders experienced by individuals with IBD and their overlap.</p><p><strong>Methods: </strong>Participants were enrolled in a prospective 3-year longitudinal study that assessed psychiatric comorbidity in immune-mediated inflammatory disease. Lifetime prevalence of psychiatric comorbidity was assessed using the Structured Clinical Interview for DSM-IV Disorders (SCID-IV), as the DSM-IV was the prevailing classification at the time of study design. Diagnosis was aligned with DSM-5 categorization where possible with available data. Psychiatric burden was categorized as no psychiatric conditions, 1, 2 or 3 or more psychiatric conditions.</p><p><strong>Results: </strong>Of 154 IBD participants (62%female, 63% Crohn's disease) 57% had at least one psychiatric comorbidity with 27% having >1 psychiatric diagnosis. The prevalence was major depressive disorder (MDD, 41.7%), anxiety disorders (39.6%; grouped as per DSM-5), substance use disorder (SUD, 16.2%), posttraumatic stress disorder (5.3%), obsessive-compulsive disorder (4.9%), and bipolar disorder (2.0%). Of participants with MDD and a comorbid psychiatric disorder, nearly half had SUD. Of those with >1 psychiatric disorder >70% had MDD and a comorbid anxiety disorder. Persons with ≥1 psychiatric comorbidity were more likely to be current smokers (<i>P</i> < .001) and to have higher IBD disease activity scores (<i>P</i> = .005) than those without a psychiatric comorbidity.</p><p><strong>Conclusions: </strong>Over half of adults with IBD had >1 diagnosed psychiatric comorbidity from a range of 10 different psychiatric disorders identified. Further research should assess the temporal relationship of IBD and the various psychiatric presentations to better understand the trajectory of co-occurrence, and therapy which may concurrently address the psychiatric disorder and the IBD.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"7 2\",\"pages\":\"otaf035\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202087/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otaf035\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:炎症性肠病(IBD)精神共病的研究主要集中在焦虑和抑郁上。本研究旨在描述IBD患者所经历的精神疾病谱系及其重叠部分。方法:参与者被纳入一项为期3年的前瞻性纵向研究,评估免疫介导的炎症性疾病的精神合并症。使用DSM-IV障碍结构化临床访谈(SCID-IV)评估精神共病的终生患病率,因为DSM-IV是研究设计时的主流分类。诊断与DSM-5分类保持一致,尽可能使用可用数据。精神负担分为无精神疾病、1种、2种或3种以上精神疾病。结果:154名IBD参与者(62%为女性,63%为克罗恩病)中,57%有至少一种精神合并症,27%有bbb1精神诊断。患病率为重度抑郁障碍(MDD, 41.7%)、焦虑障碍(39.6%;根据DSM-5分组),物质使用障碍(SUD, 16.2%),创伤后应激障碍(5.3%),强迫症(4.9%)和双相障碍(2.0%)。在重度抑郁症和共病精神障碍的参与者中,近一半患有SUD。在那些患有>精神障碍的人中,70%患有重度抑郁症和共病焦虑症。与没有精神合并症的人相比,有≥1种精神合并症的人更有可能是当前吸烟者(P P = 0.005)。结论:超过一半的IBD成年患者被诊断为10种不同精神疾病的精神共病。进一步的研究应该评估IBD与各种精神病学表现的时间关系,以更好地了解共同发生的轨迹,以及可能同时解决精神障碍和IBD的治疗方法。
The Spectrum of Psychiatric Comorbidity in Individuals With Inflammatory Bowel Disease.
Background: Research on psychiatric comorbidity in inflammatory bowel disease (IBD) has focused mostly on anxiety and depression. This study aimed to describe the spectrum of psychiatric disorders experienced by individuals with IBD and their overlap.
Methods: Participants were enrolled in a prospective 3-year longitudinal study that assessed psychiatric comorbidity in immune-mediated inflammatory disease. Lifetime prevalence of psychiatric comorbidity was assessed using the Structured Clinical Interview for DSM-IV Disorders (SCID-IV), as the DSM-IV was the prevailing classification at the time of study design. Diagnosis was aligned with DSM-5 categorization where possible with available data. Psychiatric burden was categorized as no psychiatric conditions, 1, 2 or 3 or more psychiatric conditions.
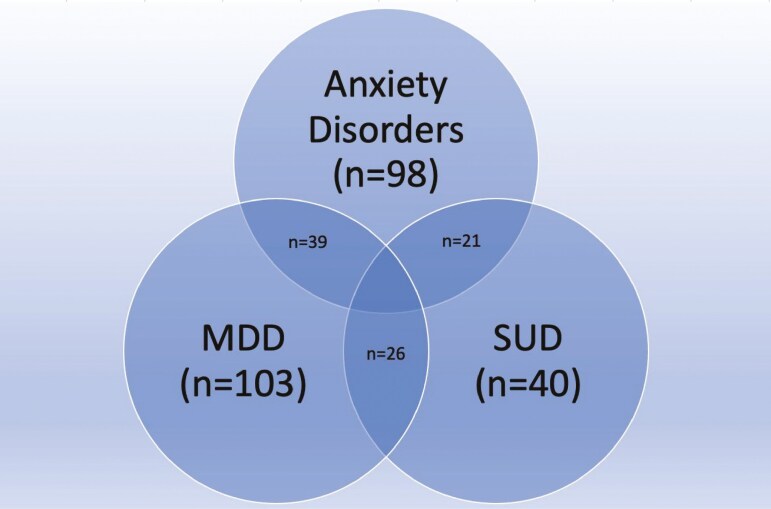
Results: Of 154 IBD participants (62%female, 63% Crohn's disease) 57% had at least one psychiatric comorbidity with 27% having >1 psychiatric diagnosis. The prevalence was major depressive disorder (MDD, 41.7%), anxiety disorders (39.6%; grouped as per DSM-5), substance use disorder (SUD, 16.2%), posttraumatic stress disorder (5.3%), obsessive-compulsive disorder (4.9%), and bipolar disorder (2.0%). Of participants with MDD and a comorbid psychiatric disorder, nearly half had SUD. Of those with >1 psychiatric disorder >70% had MDD and a comorbid anxiety disorder. Persons with ≥1 psychiatric comorbidity were more likely to be current smokers (P < .001) and to have higher IBD disease activity scores (P = .005) than those without a psychiatric comorbidity.
Conclusions: Over half of adults with IBD had >1 diagnosed psychiatric comorbidity from a range of 10 different psychiatric disorders identified. Further research should assess the temporal relationship of IBD and the various psychiatric presentations to better understand the trajectory of co-occurrence, and therapy which may concurrently address the psychiatric disorder and the IBD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


