{"title":"目前世界范围内移动脑卒中装置的应用现状及社会背景:一项调查与调查。","authors":"Masahiko Hiroki, Mototsugu Kohno, Yutaka Kohno, Masaki Misawa","doi":"10.5811/westjem.21267","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We aimed to clarify the current challenges involved in introducing and operating mobile stroke units (MSU) in new regions, considering the social background of regions with MSUs.</p><p><strong>Methods: </strong>We conducted a questionnaire survey on the operational and financial status of all active MSU programs worldwide as of March 2023, and investigated the demographic, economic, and healthcare backgrounds of areas with and without active MSUs. We compared the data for the two groups at the country, state, or city level. We then correlated data gathered from the survey and the investigation.</p><p><strong>Results: </strong>Of the 33 MSU programs contacted, 19 (59%) responded. The responding programs treated a range of 52-1,663 (median 781) patients at an MSU per year. The most commonly reported hours of operation were eight hours every weekday (5, 26%). The majority had four staff on board (11, 58%). No physicians were on board in six MSUs (32%). The catchment area radius ranged from 5-250 (median 22) kilometers. The start-up costs and subsequent annual operation costs of an MSU ranged from $0.7-1.8 million (median 1.0) and $0.7-1.7 (median 1.0) million US dollars, respectively. Reimbursement was obtained by eight (47%), with full reimbursement by two (12%). A negative gross financial balance was reported in eight MSUs (53%, of 15), and a financial challenge was reported in 17 (94%, of 18). Compared to the non-MSU group at the country level, active MSU groups had a significantly higher population, nominal gross domestic product, healthcare access and quality index, and physician density. They also had significantly lower age-standardized stroke incidence rates and age-standardized stroke disability-adjusted life year rate. The MSU operation time was significantly positively correlated with age-standardized stroke incidence rate and negatively with physician density.</p><p><strong>Conclusion: </strong>Despite facing serious financial problems, mobile stroke units currently operate around the world. However, the social context of MSUs appears relatively advanced. For future implementation of MSUs, cost-saving strategies and reimbursements should be addressed, and national or regional social backgrounds should be considered.</p>","PeriodicalId":23682,"journal":{"name":"Western Journal of Emergency Medicine","volume":"26 3","pages":"700-711"},"PeriodicalIF":2.0000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208034/pdf/","citationCount":"0","resultStr":"{\"title\":\"Practical Status and Social Background of Current Mobile Stroke Units Worldwide: A Survey and Investigation.\",\"authors\":\"Masahiko Hiroki, Mototsugu Kohno, Yutaka Kohno, Masaki Misawa\",\"doi\":\"10.5811/westjem.21267\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We aimed to clarify the current challenges involved in introducing and operating mobile stroke units (MSU) in new regions, considering the social background of regions with MSUs.</p><p><strong>Methods: </strong>We conducted a questionnaire survey on the operational and financial status of all active MSU programs worldwide as of March 2023, and investigated the demographic, economic, and healthcare backgrounds of areas with and without active MSUs. We compared the data for the two groups at the country, state, or city level. We then correlated data gathered from the survey and the investigation.</p><p><strong>Results: </strong>Of the 33 MSU programs contacted, 19 (59%) responded. The responding programs treated a range of 52-1,663 (median 781) patients at an MSU per year. The most commonly reported hours of operation were eight hours every weekday (5, 26%). The majority had four staff on board (11, 58%). No physicians were on board in six MSUs (32%). The catchment area radius ranged from 5-250 (median 22) kilometers. The start-up costs and subsequent annual operation costs of an MSU ranged from $0.7-1.8 million (median 1.0) and $0.7-1.7 (median 1.0) million US dollars, respectively. Reimbursement was obtained by eight (47%), with full reimbursement by two (12%). A negative gross financial balance was reported in eight MSUs (53%, of 15), and a financial challenge was reported in 17 (94%, of 18). Compared to the non-MSU group at the country level, active MSU groups had a significantly higher population, nominal gross domestic product, healthcare access and quality index, and physician density. They also had significantly lower age-standardized stroke incidence rates and age-standardized stroke disability-adjusted life year rate. The MSU operation time was significantly positively correlated with age-standardized stroke incidence rate and negatively with physician density.</p><p><strong>Conclusion: </strong>Despite facing serious financial problems, mobile stroke units currently operate around the world. However, the social context of MSUs appears relatively advanced. For future implementation of MSUs, cost-saving strategies and reimbursements should be addressed, and national or regional social backgrounds should be considered.</p>\",\"PeriodicalId\":23682,\"journal\":{\"name\":\"Western Journal of Emergency Medicine\",\"volume\":\"26 3\",\"pages\":\"700-711\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-05-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208034/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Western Journal of Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5811/westjem.21267\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Western Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5811/westjem.21267","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Practical Status and Social Background of Current Mobile Stroke Units Worldwide: A Survey and Investigation.
Background: We aimed to clarify the current challenges involved in introducing and operating mobile stroke units (MSU) in new regions, considering the social background of regions with MSUs.
Methods: We conducted a questionnaire survey on the operational and financial status of all active MSU programs worldwide as of March 2023, and investigated the demographic, economic, and healthcare backgrounds of areas with and without active MSUs. We compared the data for the two groups at the country, state, or city level. We then correlated data gathered from the survey and the investigation.
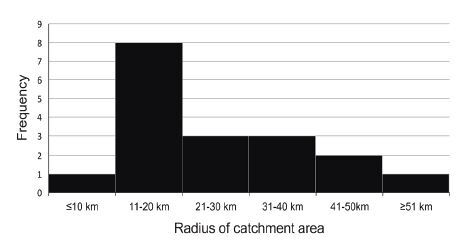
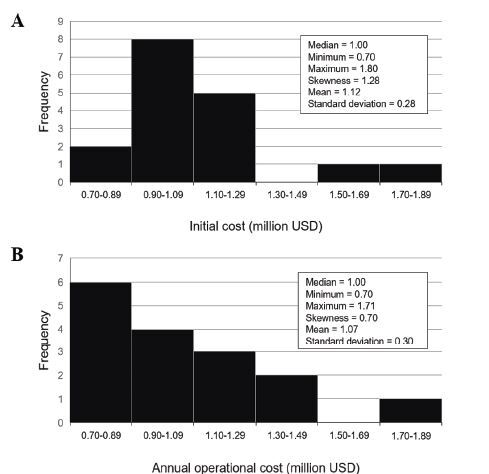
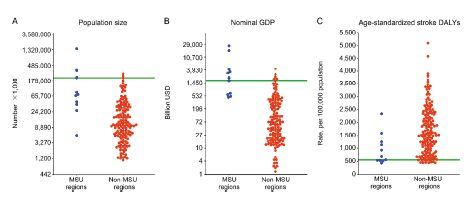
Results: Of the 33 MSU programs contacted, 19 (59%) responded. The responding programs treated a range of 52-1,663 (median 781) patients at an MSU per year. The most commonly reported hours of operation were eight hours every weekday (5, 26%). The majority had four staff on board (11, 58%). No physicians were on board in six MSUs (32%). The catchment area radius ranged from 5-250 (median 22) kilometers. The start-up costs and subsequent annual operation costs of an MSU ranged from $0.7-1.8 million (median 1.0) and $0.7-1.7 (median 1.0) million US dollars, respectively. Reimbursement was obtained by eight (47%), with full reimbursement by two (12%). A negative gross financial balance was reported in eight MSUs (53%, of 15), and a financial challenge was reported in 17 (94%, of 18). Compared to the non-MSU group at the country level, active MSU groups had a significantly higher population, nominal gross domestic product, healthcare access and quality index, and physician density. They also had significantly lower age-standardized stroke incidence rates and age-standardized stroke disability-adjusted life year rate. The MSU operation time was significantly positively correlated with age-standardized stroke incidence rate and negatively with physician density.
Conclusion: Despite facing serious financial problems, mobile stroke units currently operate around the world. However, the social context of MSUs appears relatively advanced. For future implementation of MSUs, cost-saving strategies and reimbursements should be addressed, and national or regional social backgrounds should be considered.
期刊介绍:
WestJEM focuses on how the systems and delivery of emergency care affects health, health disparities, and health outcomes in communities and populations worldwide, including the impact of social conditions on the composition of patients seeking care in emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


