Monica Majumder, Shejil Kumar, Tony Lian, Venessa H M Tsang, Meredith Oatley, Lyndal Tacon, Bruce G Robinson, Anthony Glover, Roderick J Clifton-Bligh, Matti L Gild
{"title":"lenvatinib在转移性甲状腺癌中的实际应用:澳大利亚中心的早期剂量强度和副作用概况。","authors":"Monica Majumder, Shejil Kumar, Tony Lian, Venessa H M Tsang, Meredith Oatley, Lyndal Tacon, Bruce G Robinson, Anthony Glover, Roderick J Clifton-Bligh, Matti L Gild","doi":"10.1530/EO-24-0062","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Lenvatinib is a multi-kinase inhibitor approved in radioiodine-refractory thyroid cancer based on results of a phase III trial. Real-world data have emphasised concerns regarding tolerability of the starting dose (24 mg/day) and frequency of dose-limiting treatment-related adverse effects (TRAEs). We aimed to assess early dose intensity, tolerability and efficacy using lenvatinib in metastatic thyroid cancer patients in an Australian centre.</p><p><strong>Design/methods: </strong>Retrospective medical record review was conducted of patients with advanced/metastatic differentiated, medullary and anaplastic thyroid cancer on lenvatinib at a quaternary referral centre (2014-2023).</p><p><strong>Results: </strong>64 patients were included. Median age at lenvatinib commencement was 67 years (range 38-92). 53% were female. The most common non-nodal metastases were pulmonary (86.4%) and skeletal (50.8%). Most patients commenced lenvatinib at 24 mg/day (48/53; 90.5%), with fewer than half maintaining this dose by 8 weeks (21/45; 46.7%). Those who maintained the 24 mg dose at 8 weeks were younger at lenvatinib commencement (62 years vs 71 years, <i>P</i> = 0.016) and more likely to have poorly differentiated or anaplastic thyroid cancer (42 vs 22%, <i>P</i> = 0.018). During the median 12-month follow-up, the most common TRAEs included hypertension (<i>n</i> = 37), fatigue (<i>n</i> = 35), and nausea (<i>n</i> = 18). In a subgroup of 21/35 patients with differentiated thyroid cancer, median baseline and nadir serum thyroglobulin were 305 and 21.7 μg/L (median reduction 92.5% (IQR 81.1-98.0%)). In 19/35 patients with radiological response data, the majority experienced disease control as best structural response (17/19; 93.2%).</p><p><strong>Conclusion: </strong>This real-world analysis demonstrates difficulties in maintaining early lenvatinib dose intensity, with frequent TRAEs. Greater emphasis on supportive care is needed to maximise early dose intensity and efficacy.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"5 1","pages":"e240062"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12186296/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-world lenvatinib use in metastatic thyroid cancer: early dose intensity and side effect profile in an Australian centre.\",\"authors\":\"Monica Majumder, Shejil Kumar, Tony Lian, Venessa H M Tsang, Meredith Oatley, Lyndal Tacon, Bruce G Robinson, Anthony Glover, Roderick J Clifton-Bligh, Matti L Gild\",\"doi\":\"10.1530/EO-24-0062\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Lenvatinib is a multi-kinase inhibitor approved in radioiodine-refractory thyroid cancer based on results of a phase III trial. Real-world data have emphasised concerns regarding tolerability of the starting dose (24 mg/day) and frequency of dose-limiting treatment-related adverse effects (TRAEs). We aimed to assess early dose intensity, tolerability and efficacy using lenvatinib in metastatic thyroid cancer patients in an Australian centre.</p><p><strong>Design/methods: </strong>Retrospective medical record review was conducted of patients with advanced/metastatic differentiated, medullary and anaplastic thyroid cancer on lenvatinib at a quaternary referral centre (2014-2023).</p><p><strong>Results: </strong>64 patients were included. Median age at lenvatinib commencement was 67 years (range 38-92). 53% were female. The most common non-nodal metastases were pulmonary (86.4%) and skeletal (50.8%). Most patients commenced lenvatinib at 24 mg/day (48/53; 90.5%), with fewer than half maintaining this dose by 8 weeks (21/45; 46.7%). Those who maintained the 24 mg dose at 8 weeks were younger at lenvatinib commencement (62 years vs 71 years, <i>P</i> = 0.016) and more likely to have poorly differentiated or anaplastic thyroid cancer (42 vs 22%, <i>P</i> = 0.018). During the median 12-month follow-up, the most common TRAEs included hypertension (<i>n</i> = 37), fatigue (<i>n</i> = 35), and nausea (<i>n</i> = 18). In a subgroup of 21/35 patients with differentiated thyroid cancer, median baseline and nadir serum thyroglobulin were 305 and 21.7 μg/L (median reduction 92.5% (IQR 81.1-98.0%)). In 19/35 patients with radiological response data, the majority experienced disease control as best structural response (17/19; 93.2%).</p><p><strong>Conclusion: </strong>This real-world analysis demonstrates difficulties in maintaining early lenvatinib dose intensity, with frequent TRAEs. Greater emphasis on supportive care is needed to maximise early dose intensity and efficacy.</p>\",\"PeriodicalId\":72907,\"journal\":{\"name\":\"Endocrine oncology (Bristol, England)\",\"volume\":\"5 1\",\"pages\":\"e240062\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12186296/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine oncology (Bristol, England)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1530/EO-24-0062\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-24-0062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Real-world lenvatinib use in metastatic thyroid cancer: early dose intensity and side effect profile in an Australian centre.
Objective: Lenvatinib is a multi-kinase inhibitor approved in radioiodine-refractory thyroid cancer based on results of a phase III trial. Real-world data have emphasised concerns regarding tolerability of the starting dose (24 mg/day) and frequency of dose-limiting treatment-related adverse effects (TRAEs). We aimed to assess early dose intensity, tolerability and efficacy using lenvatinib in metastatic thyroid cancer patients in an Australian centre.
Design/methods: Retrospective medical record review was conducted of patients with advanced/metastatic differentiated, medullary and anaplastic thyroid cancer on lenvatinib at a quaternary referral centre (2014-2023).
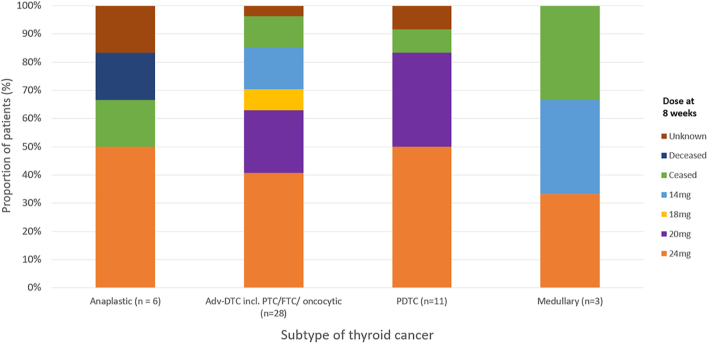
Results: 64 patients were included. Median age at lenvatinib commencement was 67 years (range 38-92). 53% were female. The most common non-nodal metastases were pulmonary (86.4%) and skeletal (50.8%). Most patients commenced lenvatinib at 24 mg/day (48/53; 90.5%), with fewer than half maintaining this dose by 8 weeks (21/45; 46.7%). Those who maintained the 24 mg dose at 8 weeks were younger at lenvatinib commencement (62 years vs 71 years, P = 0.016) and more likely to have poorly differentiated or anaplastic thyroid cancer (42 vs 22%, P = 0.018). During the median 12-month follow-up, the most common TRAEs included hypertension (n = 37), fatigue (n = 35), and nausea (n = 18). In a subgroup of 21/35 patients with differentiated thyroid cancer, median baseline and nadir serum thyroglobulin were 305 and 21.7 μg/L (median reduction 92.5% (IQR 81.1-98.0%)). In 19/35 patients with radiological response data, the majority experienced disease control as best structural response (17/19; 93.2%).
Conclusion: This real-world analysis demonstrates difficulties in maintaining early lenvatinib dose intensity, with frequent TRAEs. Greater emphasis on supportive care is needed to maximise early dose intensity and efficacy.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


