Krzysztof Wroński, Michał Tadeusz Holecki, Natalia Boguszewska, Marzena Skrzypczak-Zielińska, Jerzy Tadeusz Chudek
{"title":"骨髓发育不全和中性粒细胞减少热后硫唑嘌呤剂量增加的tpmt缺陷患者克罗恩病和银屑病关节炎-护理依从病例。","authors":"Krzysztof Wroński, Michał Tadeusz Holecki, Natalia Boguszewska, Marzena Skrzypczak-Zielińska, Jerzy Tadeusz Chudek","doi":"10.3390/clinpract15060114","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Myelotoxicity, usually manifested by moderate leukopenia (particularly neutropenia), is a well-known adverse drug reaction to azathioprine (AZA) therapy. Thiopurine methyltransferase (<i>TMPT</i>) and nucleoside diphosphate-linked moiety X-type motif 15 (<i>NUDT15)</i> genotyping are not routinely performed in patients starting AZA therapy due to their low cost-effectiveness. Additionally, the concomitant use of xanthine oxidase inhibitors and 5-aminosalicylates may slow the metabolism of 6-mercaptopurine. <b>Case Description:</b> We describe a case of a 26-year-old Caucasian man with Crohn's disease and psoriatic arthritis treated with mesalazine and AZA (100 mg daily) who developed prolonged bone marrow aplasia and neutropenic fever after increasing the daily dose of AZA from 100 to 150 mg (from 44 to 66 mg/m<sup>2</sup>), without frequent total blood count monitoring. Discontinuation of AZA, multiple transfusions of red blood cells and platelet concentrate, filgrastim, empirical antibiotic therapy, and antiviral and antifungal prophylaxis were obtained after 11 days complete recovery of bone marrow aplasia. <b>Methods:</b> Genomic DNA genotyping of coding regions of <i>TPMT</i> (exons 2-9) and <i>NUDT15</i> (exons 1-3). <b>Results:</b> Heterozygous alleles in the untranslated region (c.460G>A and c.719A>G) associated with TPMT deficiency and a benign variant (c.*7G>A) in the 3'-UTR of <i>NUDT15</i> with no effect on enzyme activity were found. <b>Conclusions:</b> This case highlights the importance of monitoring the total blood count frequently during the first weeks of treatment with moderate-to-high doses of AZA. Furthermore, the interaction between AZA and mesalazine may play a significant role in the development of prolonged bone marrow aplasia.</p>","PeriodicalId":45306,"journal":{"name":"Clinics and Practice","volume":"15 6","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12192030/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bone Marrow Aplasia and Neutropenic Fever Following Azathioprine Dose Escalation in a TPMT-Deficient Patient with Crohn's Disease and Psoriatic Arthritis-A CARE-Compliant Case.\",\"authors\":\"Krzysztof Wroński, Michał Tadeusz Holecki, Natalia Boguszewska, Marzena Skrzypczak-Zielińska, Jerzy Tadeusz Chudek\",\"doi\":\"10.3390/clinpract15060114\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Myelotoxicity, usually manifested by moderate leukopenia (particularly neutropenia), is a well-known adverse drug reaction to azathioprine (AZA) therapy. Thiopurine methyltransferase (<i>TMPT</i>) and nucleoside diphosphate-linked moiety X-type motif 15 (<i>NUDT15)</i> genotyping are not routinely performed in patients starting AZA therapy due to their low cost-effectiveness. Additionally, the concomitant use of xanthine oxidase inhibitors and 5-aminosalicylates may slow the metabolism of 6-mercaptopurine. <b>Case Description:</b> We describe a case of a 26-year-old Caucasian man with Crohn's disease and psoriatic arthritis treated with mesalazine and AZA (100 mg daily) who developed prolonged bone marrow aplasia and neutropenic fever after increasing the daily dose of AZA from 100 to 150 mg (from 44 to 66 mg/m<sup>2</sup>), without frequent total blood count monitoring. Discontinuation of AZA, multiple transfusions of red blood cells and platelet concentrate, filgrastim, empirical antibiotic therapy, and antiviral and antifungal prophylaxis were obtained after 11 days complete recovery of bone marrow aplasia. <b>Methods:</b> Genomic DNA genotyping of coding regions of <i>TPMT</i> (exons 2-9) and <i>NUDT15</i> (exons 1-3). <b>Results:</b> Heterozygous alleles in the untranslated region (c.460G>A and c.719A>G) associated with TPMT deficiency and a benign variant (c.*7G>A) in the 3'-UTR of <i>NUDT15</i> with no effect on enzyme activity were found. <b>Conclusions:</b> This case highlights the importance of monitoring the total blood count frequently during the first weeks of treatment with moderate-to-high doses of AZA. Furthermore, the interaction between AZA and mesalazine may play a significant role in the development of prolonged bone marrow aplasia.</p>\",\"PeriodicalId\":45306,\"journal\":{\"name\":\"Clinics and Practice\",\"volume\":\"15 6\",\"pages\":\"\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12192030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/clinpract15060114\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/clinpract15060114","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Bone Marrow Aplasia and Neutropenic Fever Following Azathioprine Dose Escalation in a TPMT-Deficient Patient with Crohn's Disease and Psoriatic Arthritis-A CARE-Compliant Case.
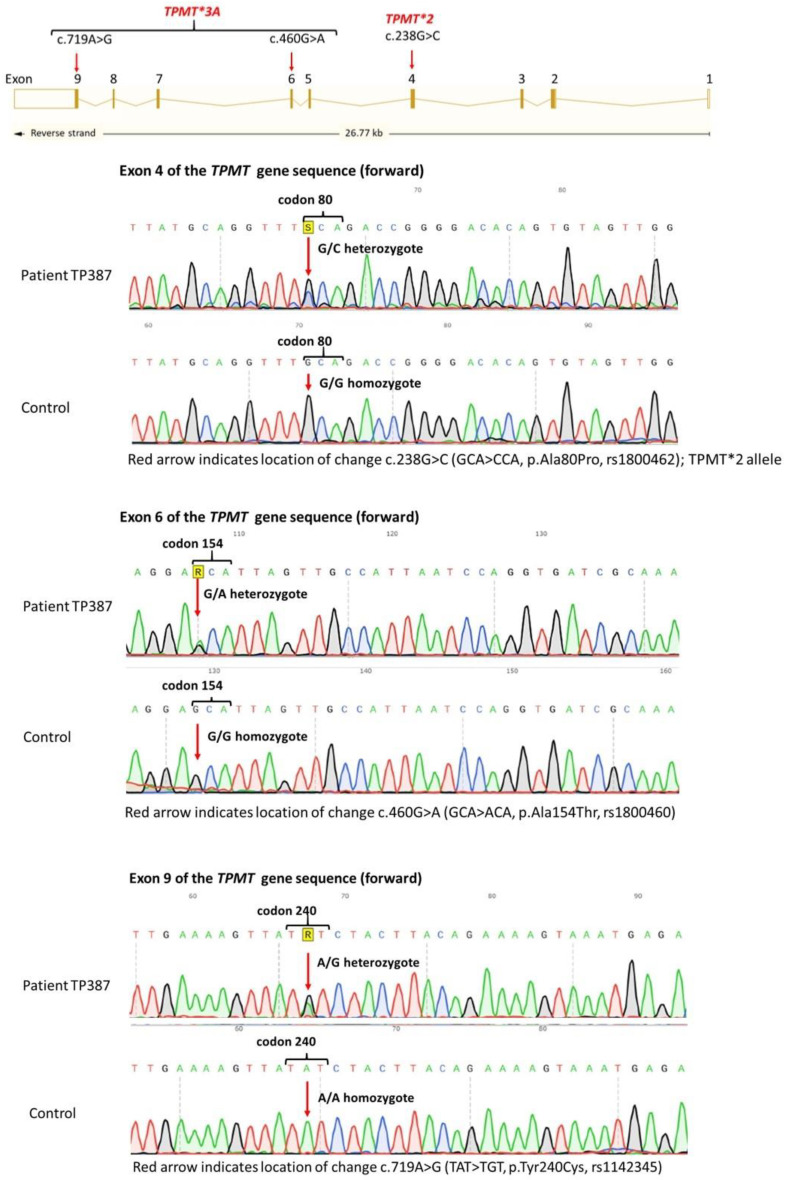
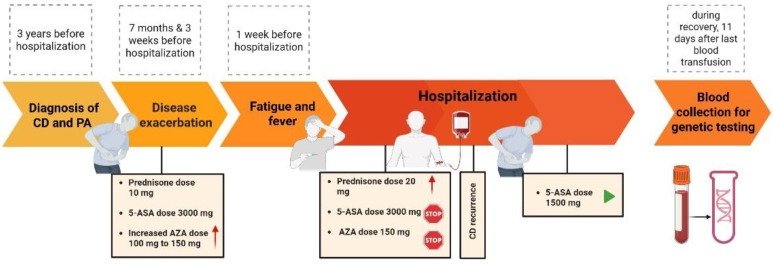
Background: Myelotoxicity, usually manifested by moderate leukopenia (particularly neutropenia), is a well-known adverse drug reaction to azathioprine (AZA) therapy. Thiopurine methyltransferase (TMPT) and nucleoside diphosphate-linked moiety X-type motif 15 (NUDT15) genotyping are not routinely performed in patients starting AZA therapy due to their low cost-effectiveness. Additionally, the concomitant use of xanthine oxidase inhibitors and 5-aminosalicylates may slow the metabolism of 6-mercaptopurine. Case Description: We describe a case of a 26-year-old Caucasian man with Crohn's disease and psoriatic arthritis treated with mesalazine and AZA (100 mg daily) who developed prolonged bone marrow aplasia and neutropenic fever after increasing the daily dose of AZA from 100 to 150 mg (from 44 to 66 mg/m2), without frequent total blood count monitoring. Discontinuation of AZA, multiple transfusions of red blood cells and platelet concentrate, filgrastim, empirical antibiotic therapy, and antiviral and antifungal prophylaxis were obtained after 11 days complete recovery of bone marrow aplasia. Methods: Genomic DNA genotyping of coding regions of TPMT (exons 2-9) and NUDT15 (exons 1-3). Results: Heterozygous alleles in the untranslated region (c.460G>A and c.719A>G) associated with TPMT deficiency and a benign variant (c.*7G>A) in the 3'-UTR of NUDT15 with no effect on enzyme activity were found. Conclusions: This case highlights the importance of monitoring the total blood count frequently during the first weeks of treatment with moderate-to-high doses of AZA. Furthermore, the interaction between AZA and mesalazine may play a significant role in the development of prolonged bone marrow aplasia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


