Christopher J Dy, Stephen J DeMartini, Eshan Sane, David M Brogan
{"title":"基于视频的臂丛神经重建后患者活动范围评估的准确性和可靠性。","authors":"Christopher J Dy, Stephen J DeMartini, Eshan Sane, David M Brogan","doi":"10.2106/JBJS.OA.25.00012","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Following surgical reconstructions considered successful, many patients with brachial plexus injuries (BPI) have limited limb motion. In addition to manual muscle testing, clinicians typically measure active range of motion (AROM). AROM measurement relies on in-person examination and manual goniometers or visual estimation, both of which are subject to interobserver variability. The purpose of this proof-of-concept study was to evaluate reliability of video-based AROM assessments. We hypothesized that video-based assessment of AROM would have high inter-rater reliability (IRR) among surgeons who perform BPI reconstruction.</p><p><strong>Methods: </strong>We video recorded a standardized examination in a convenience sample of 8 postreconstruction BPI patients performing 3 motions: elbow flexion (EF), shoulder flexion (FF), and shoulder abduction (ABD). Eight BPI surgeons were given access to the videos and instructed on how to measure AROM first visually and then digitally using ImageJ. We examined the correlation between video-based and in-person goniometry measurements and assessed IRR of visual estimates and digital goniometry using Shrout-Fleiss Intraclass 3 fixed set correlations.</p><p><strong>Results: </strong>For EF, digital goniometry had a higher correlation (r = 0.92; p < 0.01) than visual assessment (r = 0.73; p < 0.01) relative to in-person measurements. IRR for EF was 0.80 for visual assessments and 0.96 for digital assessments. For FF, digital goniometry (r = 0.80; p < 0.01) and visual assessment (r = 0.80; p < 0.01) had similar correlations relative to in-person measurements. IRR for FF was 0.95 for visual assessments and 0.99 for digital assessments. For ABD, digital goniometry had a higher correlation (r = 0.85; p < 0.01) than visual assessment (r = 0.80; p < 0.01) relative to in-person measurements. IRR for ABD was 0.91 for visual assessments and 0.96 for digital assessments.</p><p><strong>Conclusions: </strong>Using standardized footage, visual estimates and digital goniometry of patient with EF, FF, and ABD were highly reliable among BPI surgeons. Digital goniometry of AROM was slightly more reliable than visual estimates for all 3 motions.</p><p><strong>Clinical relevance: </strong>In addition to facilitating remote assessments to minimize patient travel, video-based assessments may allow opportunity to minimize reporting bias in clinical research through evaluation of results by multiple raters.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12180833/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy and Reliability of Video-Based Range-of-Motion Assessments in Postreconstruction Brachial Plexus Patients.\",\"authors\":\"Christopher J Dy, Stephen J DeMartini, Eshan Sane, David M Brogan\",\"doi\":\"10.2106/JBJS.OA.25.00012\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Following surgical reconstructions considered successful, many patients with brachial plexus injuries (BPI) have limited limb motion. In addition to manual muscle testing, clinicians typically measure active range of motion (AROM). AROM measurement relies on in-person examination and manual goniometers or visual estimation, both of which are subject to interobserver variability. The purpose of this proof-of-concept study was to evaluate reliability of video-based AROM assessments. We hypothesized that video-based assessment of AROM would have high inter-rater reliability (IRR) among surgeons who perform BPI reconstruction.</p><p><strong>Methods: </strong>We video recorded a standardized examination in a convenience sample of 8 postreconstruction BPI patients performing 3 motions: elbow flexion (EF), shoulder flexion (FF), and shoulder abduction (ABD). Eight BPI surgeons were given access to the videos and instructed on how to measure AROM first visually and then digitally using ImageJ. We examined the correlation between video-based and in-person goniometry measurements and assessed IRR of visual estimates and digital goniometry using Shrout-Fleiss Intraclass 3 fixed set correlations.</p><p><strong>Results: </strong>For EF, digital goniometry had a higher correlation (r = 0.92; p < 0.01) than visual assessment (r = 0.73; p < 0.01) relative to in-person measurements. IRR for EF was 0.80 for visual assessments and 0.96 for digital assessments. For FF, digital goniometry (r = 0.80; p < 0.01) and visual assessment (r = 0.80; p < 0.01) had similar correlations relative to in-person measurements. IRR for FF was 0.95 for visual assessments and 0.99 for digital assessments. For ABD, digital goniometry had a higher correlation (r = 0.85; p < 0.01) than visual assessment (r = 0.80; p < 0.01) relative to in-person measurements. IRR for ABD was 0.91 for visual assessments and 0.96 for digital assessments.</p><p><strong>Conclusions: </strong>Using standardized footage, visual estimates and digital goniometry of patient with EF, FF, and ABD were highly reliable among BPI surgeons. Digital goniometry of AROM was slightly more reliable than visual estimates for all 3 motions.</p><p><strong>Clinical relevance: </strong>In addition to facilitating remote assessments to minimize patient travel, video-based assessments may allow opportunity to minimize reporting bias in clinical research through evaluation of results by multiple raters.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 2\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12180833/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.25.00012\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.25.00012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Accuracy and Reliability of Video-Based Range-of-Motion Assessments in Postreconstruction Brachial Plexus Patients.
Purpose: Following surgical reconstructions considered successful, many patients with brachial plexus injuries (BPI) have limited limb motion. In addition to manual muscle testing, clinicians typically measure active range of motion (AROM). AROM measurement relies on in-person examination and manual goniometers or visual estimation, both of which are subject to interobserver variability. The purpose of this proof-of-concept study was to evaluate reliability of video-based AROM assessments. We hypothesized that video-based assessment of AROM would have high inter-rater reliability (IRR) among surgeons who perform BPI reconstruction.
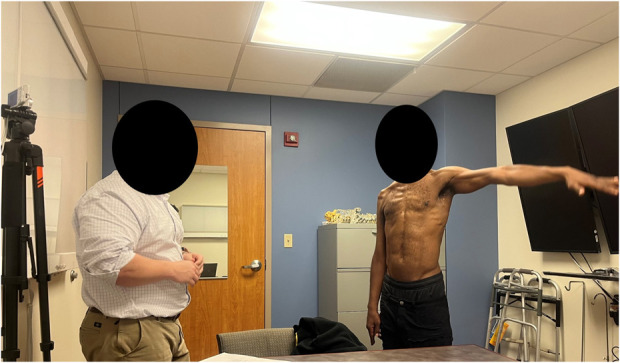
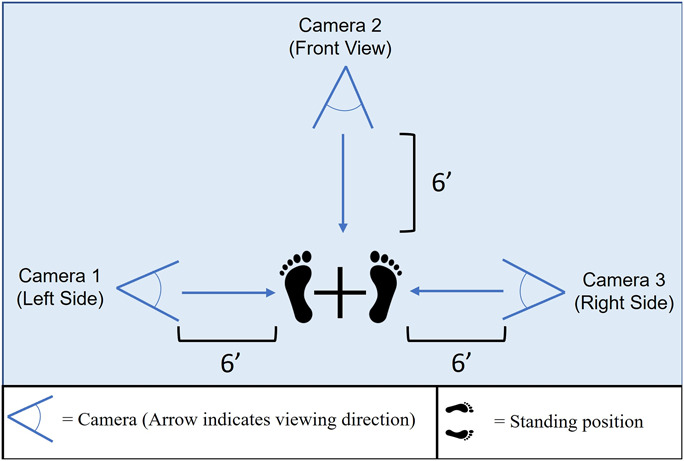
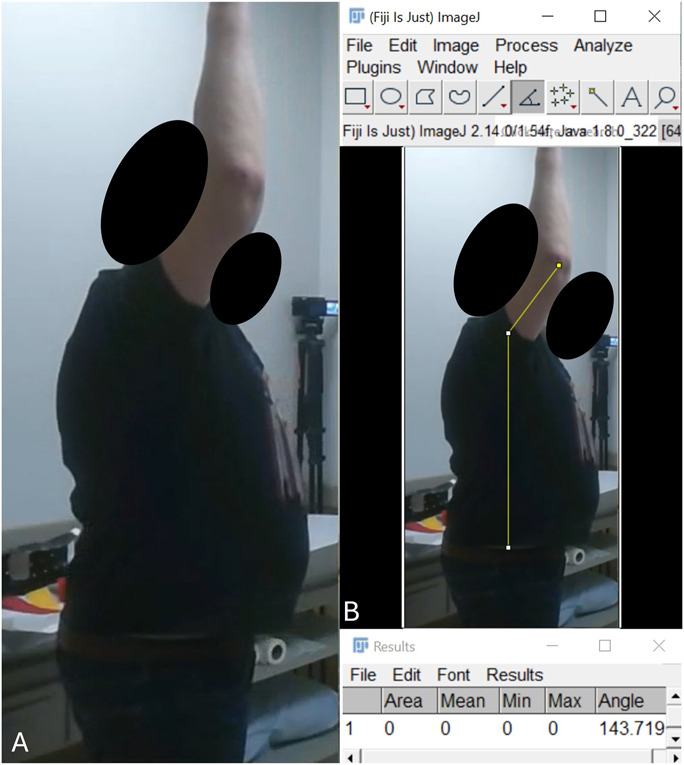
Methods: We video recorded a standardized examination in a convenience sample of 8 postreconstruction BPI patients performing 3 motions: elbow flexion (EF), shoulder flexion (FF), and shoulder abduction (ABD). Eight BPI surgeons were given access to the videos and instructed on how to measure AROM first visually and then digitally using ImageJ. We examined the correlation between video-based and in-person goniometry measurements and assessed IRR of visual estimates and digital goniometry using Shrout-Fleiss Intraclass 3 fixed set correlations.
Results: For EF, digital goniometry had a higher correlation (r = 0.92; p < 0.01) than visual assessment (r = 0.73; p < 0.01) relative to in-person measurements. IRR for EF was 0.80 for visual assessments and 0.96 for digital assessments. For FF, digital goniometry (r = 0.80; p < 0.01) and visual assessment (r = 0.80; p < 0.01) had similar correlations relative to in-person measurements. IRR for FF was 0.95 for visual assessments and 0.99 for digital assessments. For ABD, digital goniometry had a higher correlation (r = 0.85; p < 0.01) than visual assessment (r = 0.80; p < 0.01) relative to in-person measurements. IRR for ABD was 0.91 for visual assessments and 0.96 for digital assessments.
Conclusions: Using standardized footage, visual estimates and digital goniometry of patient with EF, FF, and ABD were highly reliable among BPI surgeons. Digital goniometry of AROM was slightly more reliable than visual estimates for all 3 motions.
Clinical relevance: In addition to facilitating remote assessments to minimize patient travel, video-based assessments may allow opportunity to minimize reporting bias in clinical research through evaluation of results by multiple raters.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


