Daniela Rosalba, Grazia Meneghetti, Federico Verdina, Chiara Solai, Danila Azzolina, Laura Petronio, Matteo Guaraglia, Raffaella Buscaglia, Giulio Saviolo, Gaia Furlan, Filippo Vietti, Daniele Biasucci, Savino Spadaro, Rachele Simonte, Edoardo De Robertis, Federico Longhini, Serena Penpa, Michele Ubertazzi, Elena Panuccio, Paolo Aluffi, Stefano De Cillà, Matteo Brucoli, Rosanna Vaschetto, Gianmaria Cammarota
{"title":"在接受选择性手术的儿科患者中,通过电阻抗断层扫描评估肺通气模式:来自前瞻性和观察性数据登记的见解。","authors":"Daniela Rosalba, Grazia Meneghetti, Federico Verdina, Chiara Solai, Danila Azzolina, Laura Petronio, Matteo Guaraglia, Raffaella Buscaglia, Giulio Saviolo, Gaia Furlan, Filippo Vietti, Daniele Biasucci, Savino Spadaro, Rachele Simonte, Edoardo De Robertis, Federico Longhini, Serena Penpa, Michele Ubertazzi, Elena Panuccio, Paolo Aluffi, Stefano De Cillà, Matteo Brucoli, Rosanna Vaschetto, Gianmaria Cammarota","doi":"10.1186/s44158-025-00254-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The impact of anaesthesia on lung function during paediatric surgery remains an area of active investigation. Understanding respiratory mechanics under different anaesthetic approaches is crucial for optimising pulmonary management in this vulnerable population.</p><p><strong>Objective: </strong>To assess ventilation distribution changes during different phases of anaesthesia in paediatric patients, using electrical impedance tomography (EIT).</p><p><strong>Methods: </strong>This observational study included 76 paediatric surgical patients-57 under controlled mechanical ventilation (CMV) and 19 breathing spontaneously. EIT assessed lung ventilation at multiple timepoints (T1-T6), analyzing regional distribution (ROIs) and center of ventilation (CoV).</p><p><strong>Results: </strong>In the CMV group, ventilation progressively shifted toward ventral lung regions (p < 0.0001 from T1 to T2, T3, T4, T5) with a contemporaneously reduced ventilation switching from T1 to T2 (p = 0.005), T3 (p < 0.0001), T4 (p = 0.001), and T5 (p < 0.0001). Ventilation normalised upon restoration of spontaneous breathing at the end of surgery. In the same group, CoV shifted toward non-dependent lung regions from T1 to T2, T3, T4, and T5 (p < 0.0001) and returned to baseline at T6. Overall, no modifications were observed in the spontaneous breathing group.</p><p><strong>Conclusions: </strong>In paediatric surgical patients, contrariwise to spontaneous breath where no modifications occurred, CMV induced a progressive redistribution of ventilation towards the ventral lung regions, at the expense of the dorsal zones. These changes were reversible with the recovery of spontaneous breathing.</p><p><strong>Trial registration: </strong>NCT06370507.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"5 1","pages":"34"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183812/pdf/","citationCount":"0","resultStr":"{\"title\":\"Patterns of lung aeration assessed through electrical impedance tomography in paediatric patients undergoing elective surgery: insights from a prospective and observational data-registry.\",\"authors\":\"Daniela Rosalba, Grazia Meneghetti, Federico Verdina, Chiara Solai, Danila Azzolina, Laura Petronio, Matteo Guaraglia, Raffaella Buscaglia, Giulio Saviolo, Gaia Furlan, Filippo Vietti, Daniele Biasucci, Savino Spadaro, Rachele Simonte, Edoardo De Robertis, Federico Longhini, Serena Penpa, Michele Ubertazzi, Elena Panuccio, Paolo Aluffi, Stefano De Cillà, Matteo Brucoli, Rosanna Vaschetto, Gianmaria Cammarota\",\"doi\":\"10.1186/s44158-025-00254-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The impact of anaesthesia on lung function during paediatric surgery remains an area of active investigation. Understanding respiratory mechanics under different anaesthetic approaches is crucial for optimising pulmonary management in this vulnerable population.</p><p><strong>Objective: </strong>To assess ventilation distribution changes during different phases of anaesthesia in paediatric patients, using electrical impedance tomography (EIT).</p><p><strong>Methods: </strong>This observational study included 76 paediatric surgical patients-57 under controlled mechanical ventilation (CMV) and 19 breathing spontaneously. EIT assessed lung ventilation at multiple timepoints (T1-T6), analyzing regional distribution (ROIs) and center of ventilation (CoV).</p><p><strong>Results: </strong>In the CMV group, ventilation progressively shifted toward ventral lung regions (p < 0.0001 from T1 to T2, T3, T4, T5) with a contemporaneously reduced ventilation switching from T1 to T2 (p = 0.005), T3 (p < 0.0001), T4 (p = 0.001), and T5 (p < 0.0001). Ventilation normalised upon restoration of spontaneous breathing at the end of surgery. In the same group, CoV shifted toward non-dependent lung regions from T1 to T2, T3, T4, and T5 (p < 0.0001) and returned to baseline at T6. Overall, no modifications were observed in the spontaneous breathing group.</p><p><strong>Conclusions: </strong>In paediatric surgical patients, contrariwise to spontaneous breath where no modifications occurred, CMV induced a progressive redistribution of ventilation towards the ventral lung regions, at the expense of the dorsal zones. These changes were reversible with the recovery of spontaneous breathing.</p><p><strong>Trial registration: </strong>NCT06370507.</p>\",\"PeriodicalId\":73597,\"journal\":{\"name\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"volume\":\"5 1\",\"pages\":\"34\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183812/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44158-025-00254-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-025-00254-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Patterns of lung aeration assessed through electrical impedance tomography in paediatric patients undergoing elective surgery: insights from a prospective and observational data-registry.
Background: The impact of anaesthesia on lung function during paediatric surgery remains an area of active investigation. Understanding respiratory mechanics under different anaesthetic approaches is crucial for optimising pulmonary management in this vulnerable population.
Objective: To assess ventilation distribution changes during different phases of anaesthesia in paediatric patients, using electrical impedance tomography (EIT).
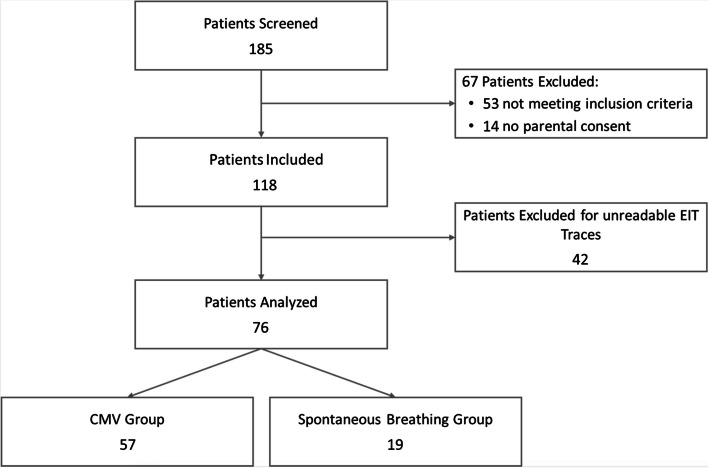
Methods: This observational study included 76 paediatric surgical patients-57 under controlled mechanical ventilation (CMV) and 19 breathing spontaneously. EIT assessed lung ventilation at multiple timepoints (T1-T6), analyzing regional distribution (ROIs) and center of ventilation (CoV).
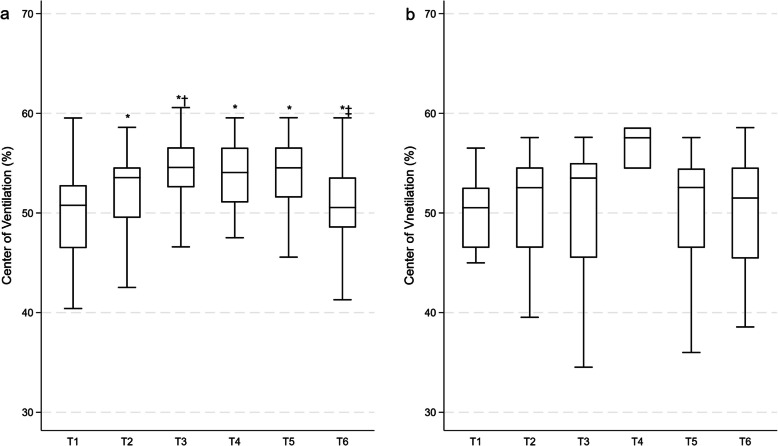
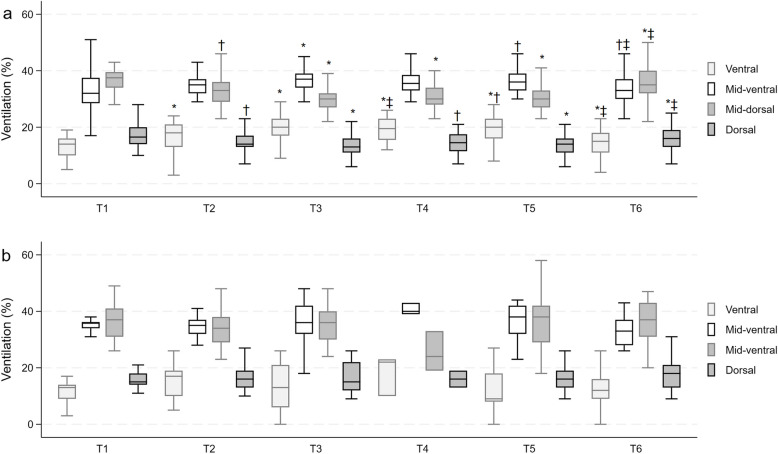
Results: In the CMV group, ventilation progressively shifted toward ventral lung regions (p < 0.0001 from T1 to T2, T3, T4, T5) with a contemporaneously reduced ventilation switching from T1 to T2 (p = 0.005), T3 (p < 0.0001), T4 (p = 0.001), and T5 (p < 0.0001). Ventilation normalised upon restoration of spontaneous breathing at the end of surgery. In the same group, CoV shifted toward non-dependent lung regions from T1 to T2, T3, T4, and T5 (p < 0.0001) and returned to baseline at T6. Overall, no modifications were observed in the spontaneous breathing group.
Conclusions: In paediatric surgical patients, contrariwise to spontaneous breath where no modifications occurred, CMV induced a progressive redistribution of ventilation towards the ventral lung regions, at the expense of the dorsal zones. These changes were reversible with the recovery of spontaneous breathing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


