Vincent Ka Chun Yan, Chengsheng Ju, Thomas MacLennan MacDonald, Isla S Mackenzie, Robert Flynn, Bryan Williams, Yang Chen, Esther W Chan, Jacob George, Li Wei
{"title":"缓释与立即释放吲达帕胺在高血压患者中的比较疗效和处方趋势:队列研究。","authors":"Vincent Ka Chun Yan, Chengsheng Ju, Thomas MacLennan MacDonald, Isla S Mackenzie, Robert Flynn, Bryan Williams, Yang Chen, Esther W Chan, Jacob George, Li Wei","doi":"10.1136/bmjmed-2024-000857","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the prescribing trends of indapamide, a thiazide-like diuretic, and the long term comparative effectiveness of modified release versus immediate release indapamide.</p><p><strong>Design: </strong>Cohort study.</p><p><strong>Setting: </strong>IQVIA Medical Research Data UK database, incorporating data from The Health Improvement Network database, 1 January 2005 to 31 December 2020.</p><p><strong>Participants: </strong>Of 1 904 289 patients with hypertension, 86 388 started indapamide treatment during the study period. 30 021 patients received modified release and 56 367 immediate release indapamide.</p><p><strong>Main outcome measures: </strong>Monthly prescribing trends of modified release and immediate release indapamide are described. A pragmatic trial was emulated to compare the five year risks of composite cardiovascular events (myocardial infarction and stroke) and death between modified release and immediate release indapamide. Intention-to-treat and per protocol effects of treatment were estimated with pooled logistic regression models. Confounding and selection bias were accounted for by multivariable adjustments and inverse probability weights.</p><p><strong>Results: </strong>1 38 414 patients who used indapamide were identified among 1 904 289 patients with hypertension. A greater increase was seen in the proportion of users of immediate release indapamide (from 0.43% in 2005 to 2.31% in 2020) than in users of modified release indapamide (from 0.71% to 0.79%). 86 388 patients (30 021 and 56 367 who started modified release and immediate release indapamide, respectively) were eligible for the trial emulation. In the intention-to-treat analysis, no difference was found in the risk of cardiovascular events (hazard ratio 0.99, 95% confidence interval (CI) 0.90 to 1.08) or death (hazard ratio 0.97, 0.92 to 1.02) between modified release and immediate release indapamide. In the per protocol analysis, a lower risk of cardiovascular events was found with modified release indapamide than with immediate release indapamide (risk difference -0.39%, 95% CI -0.71% to -0.06%; hazard ratio 0.81, 95% CI 0.68 to 0.98), which was mainly driven by myocardial infarction (risk difference -0.36%, 95% CI -0.64% to -0.08%; hazard ratio 0.80, 95% CI 0.64 to 1.01). Similar risks of death (hazard ratio 1.03, 95% CI 0.90 to 1.17) were found for the two formulations.</p><p><strong>Conclusions: </strong>In patients treated with indapamide for hypertension, starting treatment with modified release or immediate release indapamide had similar risks for cardiovascular events or all cause mortality. In an exploratory secondary analysis, sustained treatment with modified release preparations was associated with a lower the risk of cardiovascular events but not all cause mortality compared with immediate release preparations. These findings need to be confirmed in prospective studies.</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"4 1","pages":"e000857"},"PeriodicalIF":10.0000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12184341/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative effectiveness and prescribing trends of modified release versus immediate release indapamide in patients with hypertension: cohort study.\",\"authors\":\"Vincent Ka Chun Yan, Chengsheng Ju, Thomas MacLennan MacDonald, Isla S Mackenzie, Robert Flynn, Bryan Williams, Yang Chen, Esther W Chan, Jacob George, Li Wei\",\"doi\":\"10.1136/bmjmed-2024-000857\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To investigate the prescribing trends of indapamide, a thiazide-like diuretic, and the long term comparative effectiveness of modified release versus immediate release indapamide.</p><p><strong>Design: </strong>Cohort study.</p><p><strong>Setting: </strong>IQVIA Medical Research Data UK database, incorporating data from The Health Improvement Network database, 1 January 2005 to 31 December 2020.</p><p><strong>Participants: </strong>Of 1 904 289 patients with hypertension, 86 388 started indapamide treatment during the study period. 30 021 patients received modified release and 56 367 immediate release indapamide.</p><p><strong>Main outcome measures: </strong>Monthly prescribing trends of modified release and immediate release indapamide are described. A pragmatic trial was emulated to compare the five year risks of composite cardiovascular events (myocardial infarction and stroke) and death between modified release and immediate release indapamide. Intention-to-treat and per protocol effects of treatment were estimated with pooled logistic regression models. Confounding and selection bias were accounted for by multivariable adjustments and inverse probability weights.</p><p><strong>Results: </strong>1 38 414 patients who used indapamide were identified among 1 904 289 patients with hypertension. A greater increase was seen in the proportion of users of immediate release indapamide (from 0.43% in 2005 to 2.31% in 2020) than in users of modified release indapamide (from 0.71% to 0.79%). 86 388 patients (30 021 and 56 367 who started modified release and immediate release indapamide, respectively) were eligible for the trial emulation. In the intention-to-treat analysis, no difference was found in the risk of cardiovascular events (hazard ratio 0.99, 95% confidence interval (CI) 0.90 to 1.08) or death (hazard ratio 0.97, 0.92 to 1.02) between modified release and immediate release indapamide. In the per protocol analysis, a lower risk of cardiovascular events was found with modified release indapamide than with immediate release indapamide (risk difference -0.39%, 95% CI -0.71% to -0.06%; hazard ratio 0.81, 95% CI 0.68 to 0.98), which was mainly driven by myocardial infarction (risk difference -0.36%, 95% CI -0.64% to -0.08%; hazard ratio 0.80, 95% CI 0.64 to 1.01). Similar risks of death (hazard ratio 1.03, 95% CI 0.90 to 1.17) were found for the two formulations.</p><p><strong>Conclusions: </strong>In patients treated with indapamide for hypertension, starting treatment with modified release or immediate release indapamide had similar risks for cardiovascular events or all cause mortality. In an exploratory secondary analysis, sustained treatment with modified release preparations was associated with a lower the risk of cardiovascular events but not all cause mortality compared with immediate release preparations. These findings need to be confirmed in prospective studies.</p>\",\"PeriodicalId\":72433,\"journal\":{\"name\":\"BMJ medicine\",\"volume\":\"4 1\",\"pages\":\"e000857\"},\"PeriodicalIF\":10.0000,\"publicationDate\":\"2025-02-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12184341/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjmed-2024-000857\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2024-000857","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:了解噻嗪类利尿剂吲达帕胺的处方趋势,以及缓释与速释的长期疗效比较。设计:队列研究。环境:IQVIA英国医学研究数据数据库,数据来自健康改善网络数据库,2005年1月1日至2020年12月31日。参与者:在1 904 289例高血压患者中,86 388例在研究期间开始了吲达帕胺治疗。30 021例患者接受改良释放,56 367例患者接受立即释放。主要观察指标:描述吲达帕胺缓释和速释的每月处方趋势。模拟了一项实用试验,比较缓释和立即释放吲达帕胺的5年复合心血管事件(心肌梗死和卒中)和死亡风险。使用混合逻辑回归模型估计治疗意向和治疗方案的效果。通过多变量调整和逆概率权重来解释混杂和选择偏差。结果:1 904 289例高血压患者中有1 38414例使用吲达帕胺。速释吲达帕胺服用者的比例(从2005年的0.43%增加到2020年的2.31%)比缓释吲达帕胺服用者的比例(从0.71%增加到0.79%)增加得更多。86 388例患者(分别为30 021例和56 367例开始缓释吲达帕胺)符合试验模拟条件。在意向治疗分析中,未发现缓释和立即释放吲达帕胺在心血管事件风险(风险比0.99,95%可信区间(CI) 0.90 ~ 1.08)或死亡(风险比0.97,0.92 ~ 1.02)方面存在差异。在每个方案分析中,发现缓释吲达帕胺的心血管事件风险低于立即释放的吲达帕胺(风险差-0.39%,95% CI -0.71%至-0.06%;风险比0.81,95% CI 0.68 ~ 0.98),主要由心肌梗死驱动(风险差-0.36%,95% CI -0.64% ~ -0.08%;风险比0.80,95% CI 0.64 ~ 1.01)。两种配方的死亡风险相似(风险比1.03,95% CI 0.90至1.17)。结论:在接受吲达帕胺治疗高血压的患者中,缓释或立即释放吲达帕胺治疗具有相似的心血管事件或全因死亡率风险。在一项探索性的二次分析中,与立即释放制剂相比,持续使用改良释放制剂治疗与较低的心血管事件风险相关,但并非全因死亡率。这些发现需要在前瞻性研究中得到证实。
Comparative effectiveness and prescribing trends of modified release versus immediate release indapamide in patients with hypertension: cohort study.
Objective: To investigate the prescribing trends of indapamide, a thiazide-like diuretic, and the long term comparative effectiveness of modified release versus immediate release indapamide.
Design: Cohort study.
Setting: IQVIA Medical Research Data UK database, incorporating data from The Health Improvement Network database, 1 January 2005 to 31 December 2020.
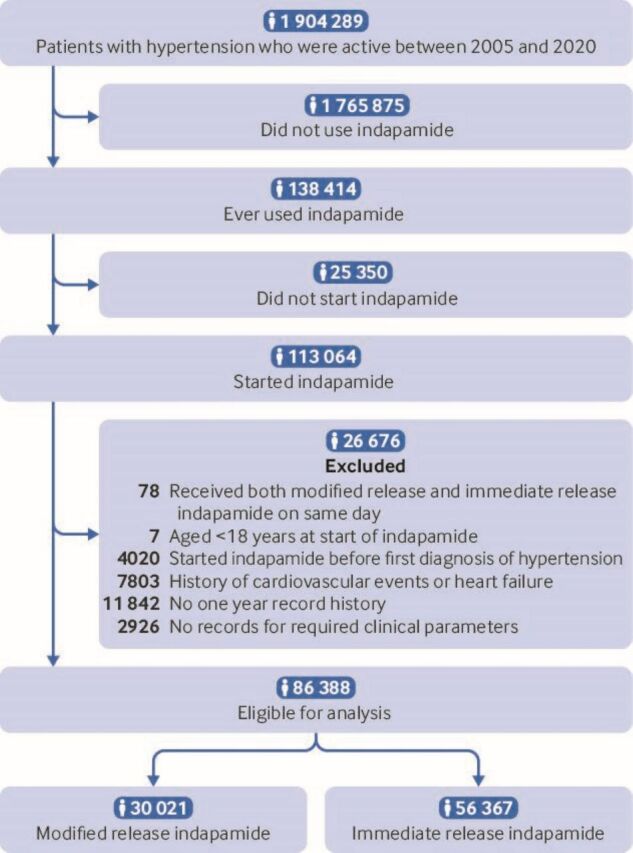
Participants: Of 1 904 289 patients with hypertension, 86 388 started indapamide treatment during the study period. 30 021 patients received modified release and 56 367 immediate release indapamide.
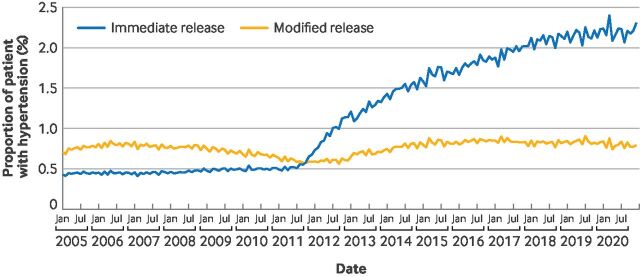
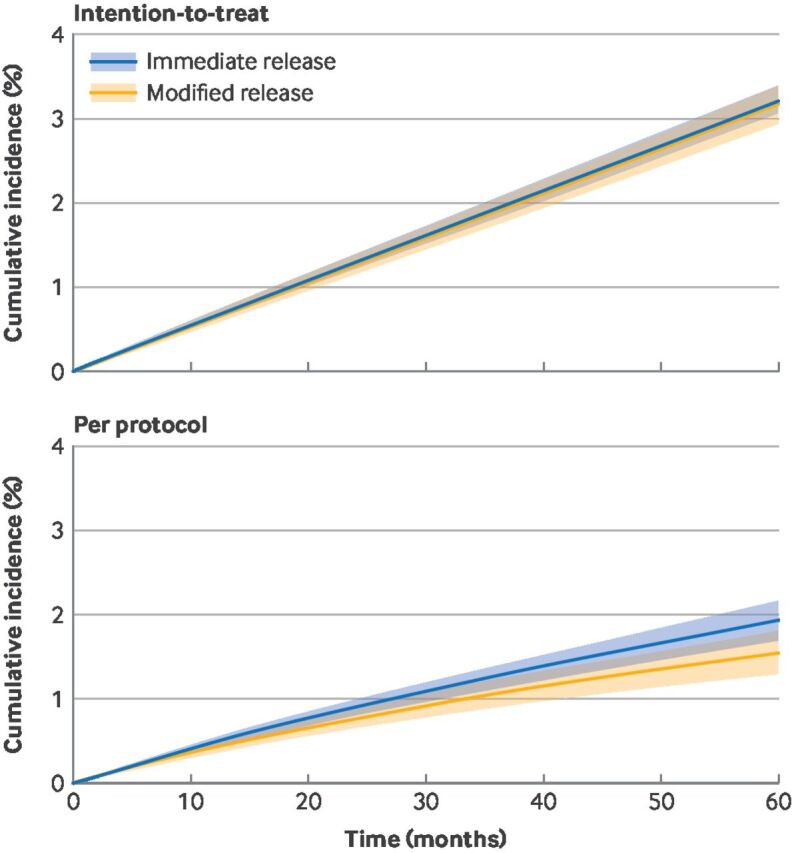
Main outcome measures: Monthly prescribing trends of modified release and immediate release indapamide are described. A pragmatic trial was emulated to compare the five year risks of composite cardiovascular events (myocardial infarction and stroke) and death between modified release and immediate release indapamide. Intention-to-treat and per protocol effects of treatment were estimated with pooled logistic regression models. Confounding and selection bias were accounted for by multivariable adjustments and inverse probability weights.
Results: 1 38 414 patients who used indapamide were identified among 1 904 289 patients with hypertension. A greater increase was seen in the proportion of users of immediate release indapamide (from 0.43% in 2005 to 2.31% in 2020) than in users of modified release indapamide (from 0.71% to 0.79%). 86 388 patients (30 021 and 56 367 who started modified release and immediate release indapamide, respectively) were eligible for the trial emulation. In the intention-to-treat analysis, no difference was found in the risk of cardiovascular events (hazard ratio 0.99, 95% confidence interval (CI) 0.90 to 1.08) or death (hazard ratio 0.97, 0.92 to 1.02) between modified release and immediate release indapamide. In the per protocol analysis, a lower risk of cardiovascular events was found with modified release indapamide than with immediate release indapamide (risk difference -0.39%, 95% CI -0.71% to -0.06%; hazard ratio 0.81, 95% CI 0.68 to 0.98), which was mainly driven by myocardial infarction (risk difference -0.36%, 95% CI -0.64% to -0.08%; hazard ratio 0.80, 95% CI 0.64 to 1.01). Similar risks of death (hazard ratio 1.03, 95% CI 0.90 to 1.17) were found for the two formulations.
Conclusions: In patients treated with indapamide for hypertension, starting treatment with modified release or immediate release indapamide had similar risks for cardiovascular events or all cause mortality. In an exploratory secondary analysis, sustained treatment with modified release preparations was associated with a lower the risk of cardiovascular events but not all cause mortality compared with immediate release preparations. These findings need to be confirmed in prospective studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


