Zofia Orzeszko, Przemysław Kasprzyk, Urszula Zawada, Mirosław Szura, Michał Spychalski
{"title":"内窥镜手术后的内窥镜手缝合:31例上、下胃肠道的早期结果(附视频)","authors":"Zofia Orzeszko, Przemysław Kasprzyk, Urszula Zawada, Mirosław Szura, Michał Spychalski","doi":"10.20452/wiitm.2025.17928","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Endoscopic hand suturing (EHS) has emerged as a promising modality in gastrointestinal (GI) endoscopic procedures. Reports on its effectiveness in clinical practice remain limited due to its recent adoption.</p><p><strong>Aim: </strong>This study aimed to describe a single- center experience regarding EHS and its outcomes.</p><p><strong>Materials and methods: </strong>This single -center retrospective study analyzed individuals that underwent advanced endoscopic procedures in the upper and lower GI tract followed by EHS. Defined features (suturing time and speed) and outcomes (postprocedural bleeding, abdominal pain) were assessed.</p><p><strong>Results: </strong>Thirty- one patients were included in the analysis. The median (interquartile range [IQR]) size of the resected lesions was 20 (20-30) mm, and the median (IQR) diameter of the sutured defects was 25 (20-31) mm. The overall suturing time was 25 minutes, with a mean (SD) speed of 1.12 (0.5) mm/min. It varied in different locations, with the fastest closure in the proximal stomach (mean [SD], 25 [13.1] min; 1.27 [0.32] mm/min) and the longest in the rectum (mean [SD], 33 [16.2] min; 0.92 [0.4] mm/min). No symptoms of GI bleeding were reported during early and 4-week follow-up. One case (4.5%) of abdominal pain was reported for the upper GI tract, and none for the lower GI tract.</p><p><strong>Conclusions: </strong>EHS is a safe and effective technique for managing defects in both gastric and rectal advanced endoscopic procedures. Its potential application in preventing post-endoscopic submucosal dissection bleeding in high-risk patients is promising. The duration and complexity of the procedure remain the challenges that may limit its broader adoption. Further research and standardized training are imperative to optimize EHS outcomes and establish it as a routine practice in endoscopic surgery.</p>","PeriodicalId":49361,"journal":{"name":"Videosurgery and Other Miniinvasive Techniques","volume":"20 1","pages":"44-50"},"PeriodicalIF":1.9000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177354/pdf/","citationCount":"0","resultStr":"{\"title\":\"Endoscopic hand suturing after advanced endoscopic procedures: early outcomes of 31 cases in the upper and lower gastrointestinal tract (with video).\",\"authors\":\"Zofia Orzeszko, Przemysław Kasprzyk, Urszula Zawada, Mirosław Szura, Michał Spychalski\",\"doi\":\"10.20452/wiitm.2025.17928\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Endoscopic hand suturing (EHS) has emerged as a promising modality in gastrointestinal (GI) endoscopic procedures. Reports on its effectiveness in clinical practice remain limited due to its recent adoption.</p><p><strong>Aim: </strong>This study aimed to describe a single- center experience regarding EHS and its outcomes.</p><p><strong>Materials and methods: </strong>This single -center retrospective study analyzed individuals that underwent advanced endoscopic procedures in the upper and lower GI tract followed by EHS. Defined features (suturing time and speed) and outcomes (postprocedural bleeding, abdominal pain) were assessed.</p><p><strong>Results: </strong>Thirty- one patients were included in the analysis. The median (interquartile range [IQR]) size of the resected lesions was 20 (20-30) mm, and the median (IQR) diameter of the sutured defects was 25 (20-31) mm. The overall suturing time was 25 minutes, with a mean (SD) speed of 1.12 (0.5) mm/min. It varied in different locations, with the fastest closure in the proximal stomach (mean [SD], 25 [13.1] min; 1.27 [0.32] mm/min) and the longest in the rectum (mean [SD], 33 [16.2] min; 0.92 [0.4] mm/min). No symptoms of GI bleeding were reported during early and 4-week follow-up. One case (4.5%) of abdominal pain was reported for the upper GI tract, and none for the lower GI tract.</p><p><strong>Conclusions: </strong>EHS is a safe and effective technique for managing defects in both gastric and rectal advanced endoscopic procedures. Its potential application in preventing post-endoscopic submucosal dissection bleeding in high-risk patients is promising. The duration and complexity of the procedure remain the challenges that may limit its broader adoption. Further research and standardized training are imperative to optimize EHS outcomes and establish it as a routine practice in endoscopic surgery.</p>\",\"PeriodicalId\":49361,\"journal\":{\"name\":\"Videosurgery and Other Miniinvasive Techniques\",\"volume\":\"20 1\",\"pages\":\"44-50\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-02-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12177354/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Videosurgery and Other Miniinvasive Techniques\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.20452/wiitm.2025.17928\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/9 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Videosurgery and Other Miniinvasive Techniques","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.20452/wiitm.2025.17928","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/9 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Endoscopic hand suturing after advanced endoscopic procedures: early outcomes of 31 cases in the upper and lower gastrointestinal tract (with video).
Introduction: Endoscopic hand suturing (EHS) has emerged as a promising modality in gastrointestinal (GI) endoscopic procedures. Reports on its effectiveness in clinical practice remain limited due to its recent adoption.
Aim: This study aimed to describe a single- center experience regarding EHS and its outcomes.
Materials and methods: This single -center retrospective study analyzed individuals that underwent advanced endoscopic procedures in the upper and lower GI tract followed by EHS. Defined features (suturing time and speed) and outcomes (postprocedural bleeding, abdominal pain) were assessed.
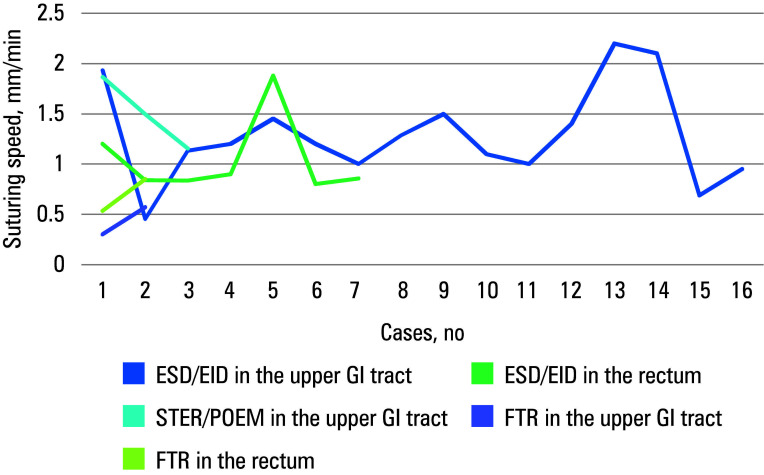
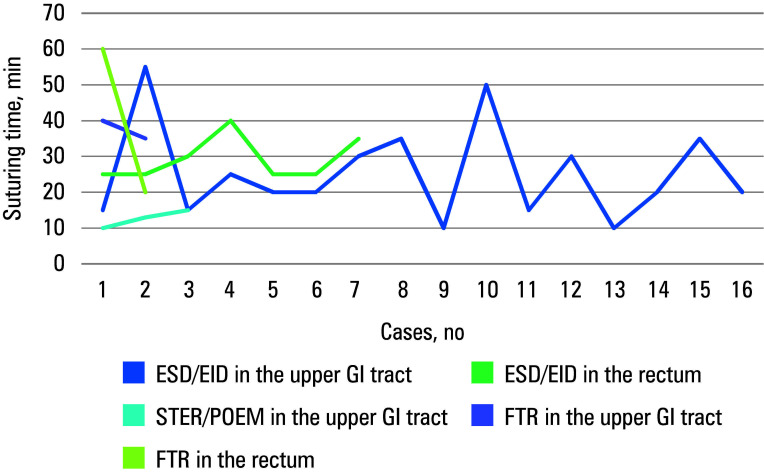
Results: Thirty- one patients were included in the analysis. The median (interquartile range [IQR]) size of the resected lesions was 20 (20-30) mm, and the median (IQR) diameter of the sutured defects was 25 (20-31) mm. The overall suturing time was 25 minutes, with a mean (SD) speed of 1.12 (0.5) mm/min. It varied in different locations, with the fastest closure in the proximal stomach (mean [SD], 25 [13.1] min; 1.27 [0.32] mm/min) and the longest in the rectum (mean [SD], 33 [16.2] min; 0.92 [0.4] mm/min). No symptoms of GI bleeding were reported during early and 4-week follow-up. One case (4.5%) of abdominal pain was reported for the upper GI tract, and none for the lower GI tract.
Conclusions: EHS is a safe and effective technique for managing defects in both gastric and rectal advanced endoscopic procedures. Its potential application in preventing post-endoscopic submucosal dissection bleeding in high-risk patients is promising. The duration and complexity of the procedure remain the challenges that may limit its broader adoption. Further research and standardized training are imperative to optimize EHS outcomes and establish it as a routine practice in endoscopic surgery.
期刊介绍:
Videosurgery and other miniinvasive techniques serves as a forum for exchange of multidisciplinary experiences in fields such as: surgery, gynaecology, urology, gastroenterology, neurosurgery, ENT surgery, cardiac surgery, anaesthesiology and radiology, as well as other branches of medicine dealing with miniinvasive techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


