Roberto A Leon-Ferre, K Dimitroff, C Yau, K V Giridhar, R Mukhtar, G Hirst, N Hylton, J Perlmutter, A DeMichele, D Yee, L van 't Veer, H Rugo, W F Symmans, M P Goetz, L Esserman, J C Boughey
{"title":"三阴性和her2阳性乳腺癌新辅助全身治疗后初始临床分期和残留癌症负担对预后的综合影响:I-SPY2随机临床试验分析","authors":"Roberto A Leon-Ferre, K Dimitroff, C Yau, K V Giridhar, R Mukhtar, G Hirst, N Hylton, J Perlmutter, A DeMichele, D Yee, L van 't Veer, H Rugo, W F Symmans, M P Goetz, L Esserman, J C Boughey","doi":"10.1186/s13058-025-02070-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Operable triple-negative (TNBC) and HER2-positive breast cancer are often treated with neoadjuvant systemic therapy (NAST). NAST response is highly prognostic, with pathologic complete response (pCR) being associated with low risk of recurrence or death. In contrast, residual disease (RD) after NAST is associated with higher risks and is an indication for escalated postoperative therapy. Recent studies suggest that tumor (T) size and nodal (N) status at diagnosis influence clinical outcomes independent of NAST response. We evaluated the impact of initial clinical stage on clinical outcomes according to response to NAST in I-SPY2.</p><p><strong>Patients and methods: </strong>Patients with stage II or III TNBC or HER2-positive breast cancer treated on the I-SPY2 trial (NCT01042379) with required data on clinical T size and N status prior to NAST, residual cancer burden (RCB) index, recurrence and survival were included. Survival outcomes, including event-free (EFS), distant recurrence-free (DRFS), and overall survival (OS), were assessed using multivariable Cox proportional hazard models.</p><p><strong>Results: </strong>Among 1,033 patients (TNBC: 638, HER2-positive: 395), the median follow-up was 4.4 years (range 0.3-10.2). 47% achieved pCR (TNBC: 44%, HER2-positive: 51%). Smaller baseline T size, but not N status, was associated with higher pCR rates. However, in those not achieving pCR, RCB class was correlated with both baseline T size and N status in TNBC, and with baseline N status (but not T size) in HER2-positive. Among patients with RD, larger baseline T size was independently associated with worse EFS and DRFS in TNBC and HER2-positive, and with OS in TNBC; while N status was associated with EFS and DRFS in TNBC on univariate analysis only. We did not identify an association between baseline T size or N status and outcomes in patients achieving pCR.</p><p><strong>Conclusions: </strong>Tumor size at diagnosis remained an independent prognostic factor in patients with TNBC and HER2-positive breast cancer with RD after NAST. In contrast, patients achieving pCR had excellent outcomes regardless of initial disease extent, supporting the relevance of pCR as a surrogate endpoint in breast cancer.</p><p><strong>Trial registration: </strong>I-SPY 2 TRIAL beginning December 31, 2009: Neoadjuvant and Personalized Adaptive Novel Agents to Treat Breast Cancer (I-SPY 2), NCT01042379.</p>","PeriodicalId":49227,"journal":{"name":"Breast Cancer Research","volume":"27 1","pages":"115"},"PeriodicalIF":5.6000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183850/pdf/","citationCount":"0","resultStr":"{\"title\":\"Combined prognostic impact of initial clinical stage and residual cancer burden after neoadjuvant systemic therapy in triple-negative and HER2-positive breast cancer: an analysis of the I-SPY2 randomized clinical trial.\",\"authors\":\"Roberto A Leon-Ferre, K Dimitroff, C Yau, K V Giridhar, R Mukhtar, G Hirst, N Hylton, J Perlmutter, A DeMichele, D Yee, L van 't Veer, H Rugo, W F Symmans, M P Goetz, L Esserman, J C Boughey\",\"doi\":\"10.1186/s13058-025-02070-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Operable triple-negative (TNBC) and HER2-positive breast cancer are often treated with neoadjuvant systemic therapy (NAST). NAST response is highly prognostic, with pathologic complete response (pCR) being associated with low risk of recurrence or death. In contrast, residual disease (RD) after NAST is associated with higher risks and is an indication for escalated postoperative therapy. Recent studies suggest that tumor (T) size and nodal (N) status at diagnosis influence clinical outcomes independent of NAST response. We evaluated the impact of initial clinical stage on clinical outcomes according to response to NAST in I-SPY2.</p><p><strong>Patients and methods: </strong>Patients with stage II or III TNBC or HER2-positive breast cancer treated on the I-SPY2 trial (NCT01042379) with required data on clinical T size and N status prior to NAST, residual cancer burden (RCB) index, recurrence and survival were included. Survival outcomes, including event-free (EFS), distant recurrence-free (DRFS), and overall survival (OS), were assessed using multivariable Cox proportional hazard models.</p><p><strong>Results: </strong>Among 1,033 patients (TNBC: 638, HER2-positive: 395), the median follow-up was 4.4 years (range 0.3-10.2). 47% achieved pCR (TNBC: 44%, HER2-positive: 51%). Smaller baseline T size, but not N status, was associated with higher pCR rates. However, in those not achieving pCR, RCB class was correlated with both baseline T size and N status in TNBC, and with baseline N status (but not T size) in HER2-positive. Among patients with RD, larger baseline T size was independently associated with worse EFS and DRFS in TNBC and HER2-positive, and with OS in TNBC; while N status was associated with EFS and DRFS in TNBC on univariate analysis only. We did not identify an association between baseline T size or N status and outcomes in patients achieving pCR.</p><p><strong>Conclusions: </strong>Tumor size at diagnosis remained an independent prognostic factor in patients with TNBC and HER2-positive breast cancer with RD after NAST. In contrast, patients achieving pCR had excellent outcomes regardless of initial disease extent, supporting the relevance of pCR as a surrogate endpoint in breast cancer.</p><p><strong>Trial registration: </strong>I-SPY 2 TRIAL beginning December 31, 2009: Neoadjuvant and Personalized Adaptive Novel Agents to Treat Breast Cancer (I-SPY 2), NCT01042379.</p>\",\"PeriodicalId\":49227,\"journal\":{\"name\":\"Breast Cancer Research\",\"volume\":\"27 1\",\"pages\":\"115\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2025-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183850/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Breast Cancer Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13058-025-02070-1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13058-025-02070-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Combined prognostic impact of initial clinical stage and residual cancer burden after neoadjuvant systemic therapy in triple-negative and HER2-positive breast cancer: an analysis of the I-SPY2 randomized clinical trial.
Background: Operable triple-negative (TNBC) and HER2-positive breast cancer are often treated with neoadjuvant systemic therapy (NAST). NAST response is highly prognostic, with pathologic complete response (pCR) being associated with low risk of recurrence or death. In contrast, residual disease (RD) after NAST is associated with higher risks and is an indication for escalated postoperative therapy. Recent studies suggest that tumor (T) size and nodal (N) status at diagnosis influence clinical outcomes independent of NAST response. We evaluated the impact of initial clinical stage on clinical outcomes according to response to NAST in I-SPY2.
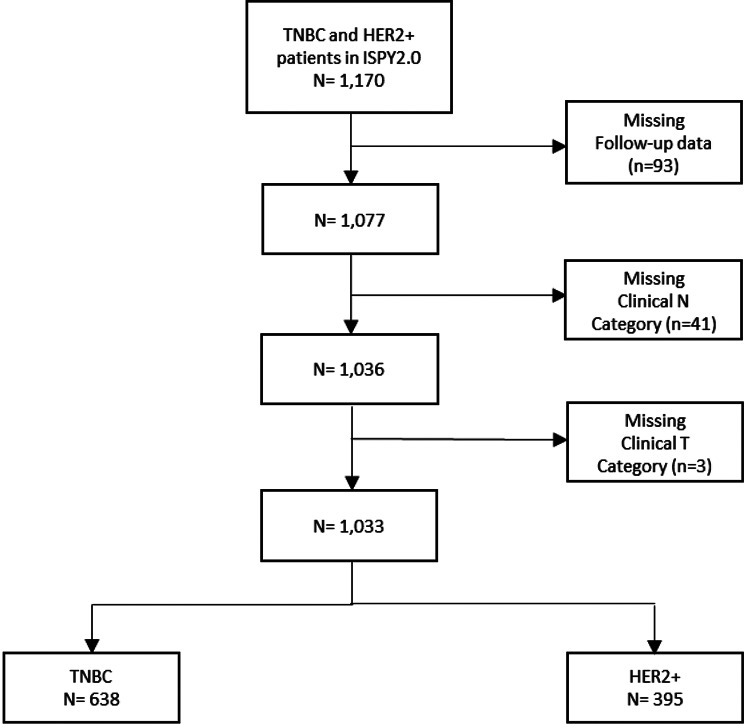
Patients and methods: Patients with stage II or III TNBC or HER2-positive breast cancer treated on the I-SPY2 trial (NCT01042379) with required data on clinical T size and N status prior to NAST, residual cancer burden (RCB) index, recurrence and survival were included. Survival outcomes, including event-free (EFS), distant recurrence-free (DRFS), and overall survival (OS), were assessed using multivariable Cox proportional hazard models.
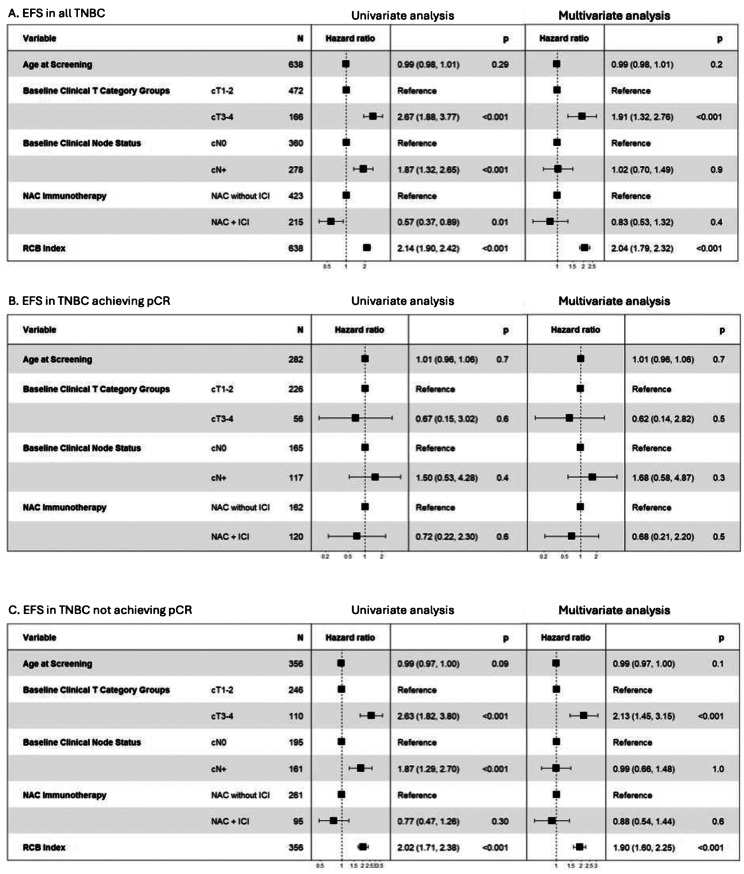
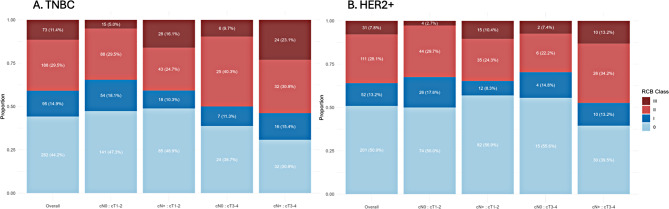
Results: Among 1,033 patients (TNBC: 638, HER2-positive: 395), the median follow-up was 4.4 years (range 0.3-10.2). 47% achieved pCR (TNBC: 44%, HER2-positive: 51%). Smaller baseline T size, but not N status, was associated with higher pCR rates. However, in those not achieving pCR, RCB class was correlated with both baseline T size and N status in TNBC, and with baseline N status (but not T size) in HER2-positive. Among patients with RD, larger baseline T size was independently associated with worse EFS and DRFS in TNBC and HER2-positive, and with OS in TNBC; while N status was associated with EFS and DRFS in TNBC on univariate analysis only. We did not identify an association between baseline T size or N status and outcomes in patients achieving pCR.
Conclusions: Tumor size at diagnosis remained an independent prognostic factor in patients with TNBC and HER2-positive breast cancer with RD after NAST. In contrast, patients achieving pCR had excellent outcomes regardless of initial disease extent, supporting the relevance of pCR as a surrogate endpoint in breast cancer.
Trial registration: I-SPY 2 TRIAL beginning December 31, 2009: Neoadjuvant and Personalized Adaptive Novel Agents to Treat Breast Cancer (I-SPY 2), NCT01042379.
期刊介绍:
Breast Cancer Research, an international, peer-reviewed online journal, publishes original research, reviews, editorials, and reports. It features open-access research articles of exceptional interest across all areas of biology and medicine relevant to breast cancer. This includes normal mammary gland biology, with a special emphasis on the genetic, biochemical, and cellular basis of breast cancer. In addition to basic research, the journal covers preclinical, translational, and clinical studies with a biological basis, including Phase I and Phase II trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


