{"title":"分离性三尖瓣心内膜炎的手术干预——细化患者的选择。","authors":"Ali Hage, Rami Abazid, Fadi Hage, Shevan Bladia, Linrui Guo, Nikolaos Tzemos","doi":"10.1055/s-0045-1808059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we analyzed various clinical and imaging factors of patients with isolated tricuspid valve infective endocarditis (TVIE) who have undergone surgical intervention, and assessed short- and long-term outcomes after surgery.</p><p><strong>Methods: </strong>We retrospectively enrolled 26 patients diagnosed with definite isolated TVIE and underwent surgical intervention between February 2004 and August 2019. We collected patients' demographics, preoperative and postoperative data. The primary outcomes were death and a composite of the following: death, readmission with right-sided heart failure, or recurrent endocarditis.</p><p><strong>Results: </strong>A total of 29 isolated tricuspid valve surgical interventions were performed on 26 patients. The mean age was 38.6 ± 12.3 years. In total, 22/29 (75.8%) of TVIE were related to <i>Staphylococcus aureus</i> and 4/29 (13.8%) were secondary to fungal infection. During a follow-up of 5.4 ± 3.7 years, there were 9 (34.6%) deaths and 15 (57.7%) composite outcomes. Multivariable Cox regression analysis showed that male sex (hazard ratio [HR]: 16.68, 95% confidence interval [CI]: 1.63-170.34, <i>p</i> = 0.018) and intravenous drug users (IVDU) (HR: 25.66, 95% CI: 1.87-352.79, <i>p</i> = 0.015) are significantly associated with increase death; on the other hand, higher level of preoperative hemoglobin and preoperative left ventricular ejection fraction (LVEF) was found to have decreased hazard of death: HR: 0.90, 95% CI: 0.82-0.99, <i>p</i> = 0.033 and HR: 0.92, 95% CI: 0.86-0.98, <i>p</i> = 0.013, respectively.</p><p><strong>Conclusion: </strong>In our institution, surgical intervention for isolated TVIE has a mortality rate of 34.6%. Men, a history of IVDU, lower preoperative hemoglobin levels, and reduced LVEF were significant predictors of postsurgical mortality. Earlier surgical intervention for TVIE before the development of anemia or impaired LV systolic function may have a potential survival benefit.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"15 2","pages":"74-79"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178669/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Intervention for Isolated Tricuspid Valve Endocarditis-Refining Patients' Selection.\",\"authors\":\"Ali Hage, Rami Abazid, Fadi Hage, Shevan Bladia, Linrui Guo, Nikolaos Tzemos\",\"doi\":\"10.1055/s-0045-1808059\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In this study, we analyzed various clinical and imaging factors of patients with isolated tricuspid valve infective endocarditis (TVIE) who have undergone surgical intervention, and assessed short- and long-term outcomes after surgery.</p><p><strong>Methods: </strong>We retrospectively enrolled 26 patients diagnosed with definite isolated TVIE and underwent surgical intervention between February 2004 and August 2019. We collected patients' demographics, preoperative and postoperative data. The primary outcomes were death and a composite of the following: death, readmission with right-sided heart failure, or recurrent endocarditis.</p><p><strong>Results: </strong>A total of 29 isolated tricuspid valve surgical interventions were performed on 26 patients. The mean age was 38.6 ± 12.3 years. In total, 22/29 (75.8%) of TVIE were related to <i>Staphylococcus aureus</i> and 4/29 (13.8%) were secondary to fungal infection. During a follow-up of 5.4 ± 3.7 years, there were 9 (34.6%) deaths and 15 (57.7%) composite outcomes. Multivariable Cox regression analysis showed that male sex (hazard ratio [HR]: 16.68, 95% confidence interval [CI]: 1.63-170.34, <i>p</i> = 0.018) and intravenous drug users (IVDU) (HR: 25.66, 95% CI: 1.87-352.79, <i>p</i> = 0.015) are significantly associated with increase death; on the other hand, higher level of preoperative hemoglobin and preoperative left ventricular ejection fraction (LVEF) was found to have decreased hazard of death: HR: 0.90, 95% CI: 0.82-0.99, <i>p</i> = 0.033 and HR: 0.92, 95% CI: 0.86-0.98, <i>p</i> = 0.013, respectively.</p><p><strong>Conclusion: </strong>In our institution, surgical intervention for isolated TVIE has a mortality rate of 34.6%. Men, a history of IVDU, lower preoperative hemoglobin levels, and reduced LVEF were significant predictors of postsurgical mortality. Earlier surgical intervention for TVIE before the development of anemia or impaired LV systolic function may have a potential survival benefit.</p>\",\"PeriodicalId\":32889,\"journal\":{\"name\":\"Avicenna Journal of Medicine\",\"volume\":\"15 2\",\"pages\":\"74-79\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12178669/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Avicenna Journal of Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0045-1808059\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1808059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:在本研究中,我们分析了孤立性三尖瓣感染性心内膜炎(TVIE)患者接受手术干预的各种临床和影像学因素,并评估了手术后的短期和长期预后。方法:回顾性纳入26例确诊为孤立性TVIE并于2004年2月至2019年8月接受手术治疗的患者。我们收集了患者的人口统计学、术前和术后数据。主要结局为死亡和以下综合结局:死亡、右侧心力衰竭再入院或复发性心内膜炎。结果:26例患者共行29例离体三尖瓣手术。平均年龄38.6±12.3岁。其中22/29例(75.8%)与金黄色葡萄球菌相关,4/29例(13.8%)继发于真菌感染。随访5.4±3.7年,死亡9例(34.6%),综合结局15例(57.7%)。多变量Cox回归分析显示,男性(风险比[HR]: 16.68, 95%可信区间[CI]: 1.63 ~ 170.34, p = 0.018)和静脉吸毒者(IVDU)(风险比:25.66,95% CI: 1.87 ~ 352.79, p = 0.015)与死亡增加显著相关;另一方面,较高的术前血红蛋白和术前左室射血分数(LVEF)水平降低了死亡风险:HR: 0.90, 95% CI: 0.82 ~ 0.99, p = 0.033; HR: 0.92, 95% CI: 0.86 ~ 0.98, p = 0.013。结论:本院孤立性TVIE手术治疗死亡率为34.6%。男性、IVDU病史、较低的术前血红蛋白水平和较低的LVEF是术后死亡率的重要预测因素。在发生贫血或左室收缩功能受损之前对TVIE进行早期手术干预可能有潜在的生存益处。
Surgical Intervention for Isolated Tricuspid Valve Endocarditis-Refining Patients' Selection.
Background: In this study, we analyzed various clinical and imaging factors of patients with isolated tricuspid valve infective endocarditis (TVIE) who have undergone surgical intervention, and assessed short- and long-term outcomes after surgery.
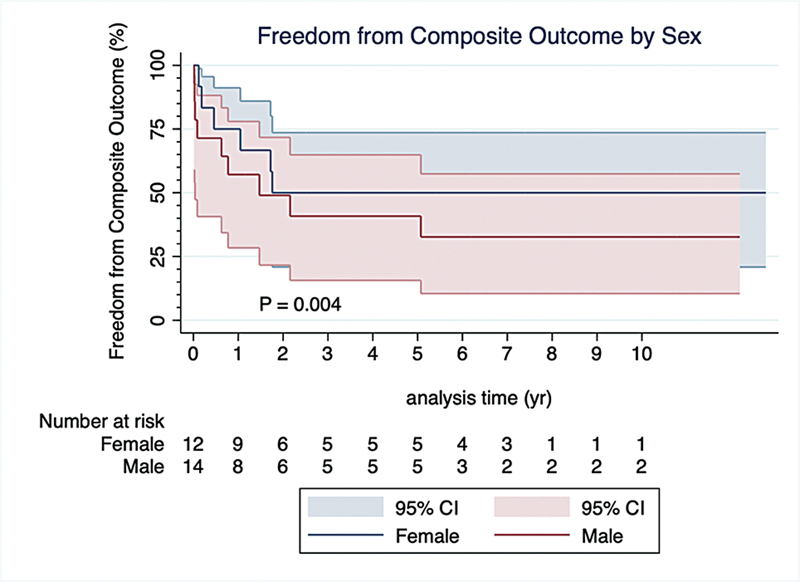
Methods: We retrospectively enrolled 26 patients diagnosed with definite isolated TVIE and underwent surgical intervention between February 2004 and August 2019. We collected patients' demographics, preoperative and postoperative data. The primary outcomes were death and a composite of the following: death, readmission with right-sided heart failure, or recurrent endocarditis.
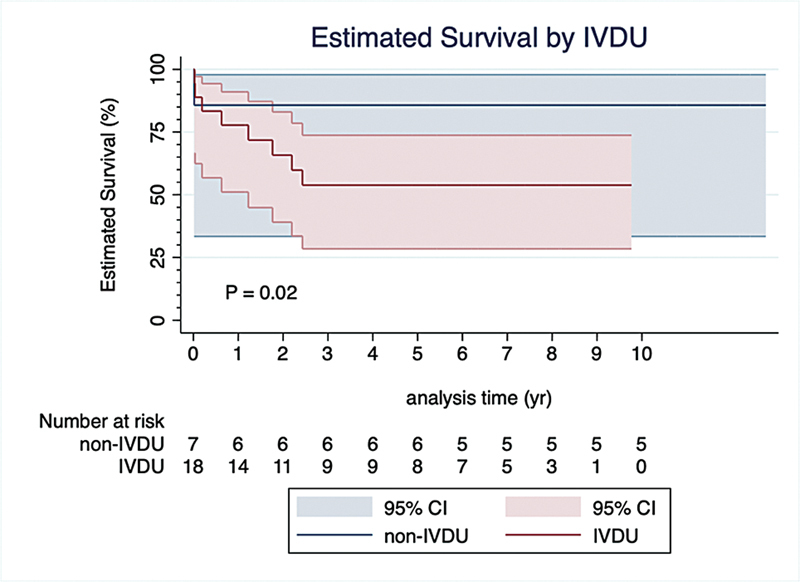
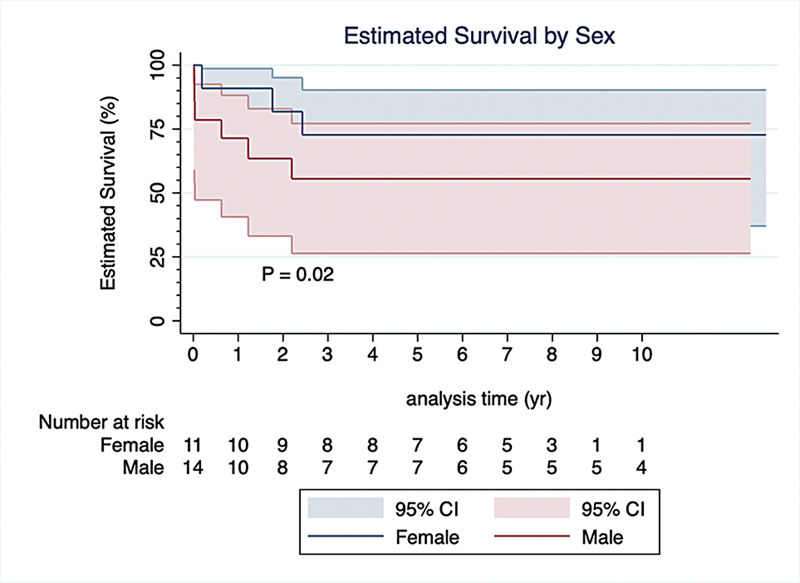
Results: A total of 29 isolated tricuspid valve surgical interventions were performed on 26 patients. The mean age was 38.6 ± 12.3 years. In total, 22/29 (75.8%) of TVIE were related to Staphylococcus aureus and 4/29 (13.8%) were secondary to fungal infection. During a follow-up of 5.4 ± 3.7 years, there were 9 (34.6%) deaths and 15 (57.7%) composite outcomes. Multivariable Cox regression analysis showed that male sex (hazard ratio [HR]: 16.68, 95% confidence interval [CI]: 1.63-170.34, p = 0.018) and intravenous drug users (IVDU) (HR: 25.66, 95% CI: 1.87-352.79, p = 0.015) are significantly associated with increase death; on the other hand, higher level of preoperative hemoglobin and preoperative left ventricular ejection fraction (LVEF) was found to have decreased hazard of death: HR: 0.90, 95% CI: 0.82-0.99, p = 0.033 and HR: 0.92, 95% CI: 0.86-0.98, p = 0.013, respectively.
Conclusion: In our institution, surgical intervention for isolated TVIE has a mortality rate of 34.6%. Men, a history of IVDU, lower preoperative hemoglobin levels, and reduced LVEF were significant predictors of postsurgical mortality. Earlier surgical intervention for TVIE before the development of anemia or impaired LV systolic function may have a potential survival benefit.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


