Suzanne J Baron, Serge Korjian, C Michael Gibson, Matthew R Reynolds
{"title":"CADScor系统在急诊科胸痛低危患者中的成本效益","authors":"Suzanne J Baron, Serge Korjian, C Michael Gibson, Matthew R Reynolds","doi":"10.1007/s41669-025-00590-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Studies have shown that up to 13% of patients presenting to the emergency department (ED) with low-risk chest pain receive further cardiac testing beyond an electrocardiogram and serial cardiac enzymes. The CADScor System is a US Food and Drug Administration (FDA)-cleared device that uses ultra-sensitive phonocardiography to evaluate the risk of significant coronary artery disease (CAD).</p><p><strong>Objective: </strong>To evaluate the relative cost-effectiveness of the CADScor system compared with other diagnostic modalities for the evaluation of low-risk chest pain in patients presenting to the ED in the USA.</p><p><strong>Methods: </strong>A two-part economic model, consisting of a decision analytic tree followed by a short-term Markov model, was developed to compare 1-year costs and outcomes (e.g., quality-adjusted life year [QALY], false-negatives, and related cardiac events) associated with the CADScor System as the first-line test versus other noninvasive cardiac tests from the perspective of the US healthcare system (TreeAge Pro). Model inputs were derived from literature, and costs for treatment strategies were calculated from average US reimbursements associated with Current Procedural Terminology and Medicare Severity Diagnosis Related Group codes. Values were reported in 2023 US dollars (USD). Parameter uncertainty was assessed through a series of deterministic and one-way sensitivity analyses.</p><p><strong>Results: </strong>Base case results demonstrated that a CADScor-First strategy was cost saving compared with other noninvasive cardiac tests without a substantial difference in adverse events. Economic results were consistent when coronary artery disease (CAD) prevalence rates were varied from 2 to 30% and across a variety of sensitivity analyses. The overall cost savings were estimated to be $7.3-15.3 million USD per 10,000 patients with low-risk chest pain.</p><p><strong>Conclusions: </strong>Use of a CADScor-First strategy in the evaluation of patients with low-risk chest pain presenting to the ED may result in substantial cost savings for the US healthcare system. More research is needed to understand the long-term costs and outcomes of this strategy.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"805-814"},"PeriodicalIF":2.1000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401830/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness of the CADScor System in Low-Risk Patients Presenting to the Emergency Department with Chest Pain.\",\"authors\":\"Suzanne J Baron, Serge Korjian, C Michael Gibson, Matthew R Reynolds\",\"doi\":\"10.1007/s41669-025-00590-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Studies have shown that up to 13% of patients presenting to the emergency department (ED) with low-risk chest pain receive further cardiac testing beyond an electrocardiogram and serial cardiac enzymes. The CADScor System is a US Food and Drug Administration (FDA)-cleared device that uses ultra-sensitive phonocardiography to evaluate the risk of significant coronary artery disease (CAD).</p><p><strong>Objective: </strong>To evaluate the relative cost-effectiveness of the CADScor system compared with other diagnostic modalities for the evaluation of low-risk chest pain in patients presenting to the ED in the USA.</p><p><strong>Methods: </strong>A two-part economic model, consisting of a decision analytic tree followed by a short-term Markov model, was developed to compare 1-year costs and outcomes (e.g., quality-adjusted life year [QALY], false-negatives, and related cardiac events) associated with the CADScor System as the first-line test versus other noninvasive cardiac tests from the perspective of the US healthcare system (TreeAge Pro). Model inputs were derived from literature, and costs for treatment strategies were calculated from average US reimbursements associated with Current Procedural Terminology and Medicare Severity Diagnosis Related Group codes. Values were reported in 2023 US dollars (USD). Parameter uncertainty was assessed through a series of deterministic and one-way sensitivity analyses.</p><p><strong>Results: </strong>Base case results demonstrated that a CADScor-First strategy was cost saving compared with other noninvasive cardiac tests without a substantial difference in adverse events. Economic results were consistent when coronary artery disease (CAD) prevalence rates were varied from 2 to 30% and across a variety of sensitivity analyses. The overall cost savings were estimated to be $7.3-15.3 million USD per 10,000 patients with low-risk chest pain.</p><p><strong>Conclusions: </strong>Use of a CADScor-First strategy in the evaluation of patients with low-risk chest pain presenting to the ED may result in substantial cost savings for the US healthcare system. More research is needed to understand the long-term costs and outcomes of this strategy.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"805-814\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401830/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-025-00590-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00590-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost-Effectiveness of the CADScor System in Low-Risk Patients Presenting to the Emergency Department with Chest Pain.
Background: Studies have shown that up to 13% of patients presenting to the emergency department (ED) with low-risk chest pain receive further cardiac testing beyond an electrocardiogram and serial cardiac enzymes. The CADScor System is a US Food and Drug Administration (FDA)-cleared device that uses ultra-sensitive phonocardiography to evaluate the risk of significant coronary artery disease (CAD).
Objective: To evaluate the relative cost-effectiveness of the CADScor system compared with other diagnostic modalities for the evaluation of low-risk chest pain in patients presenting to the ED in the USA.
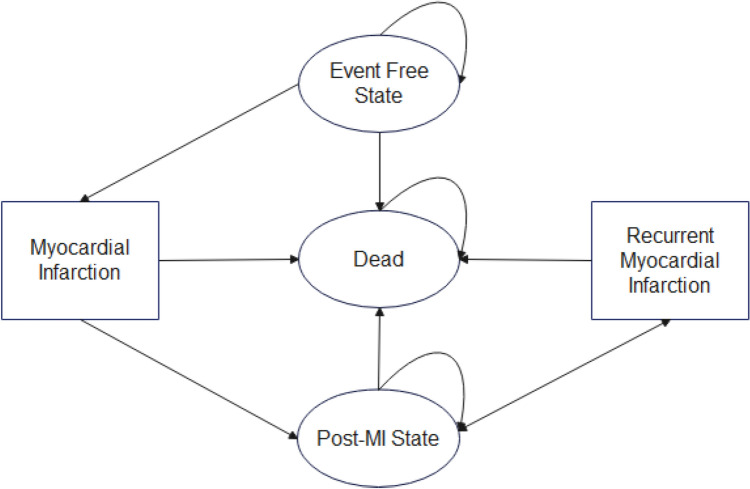
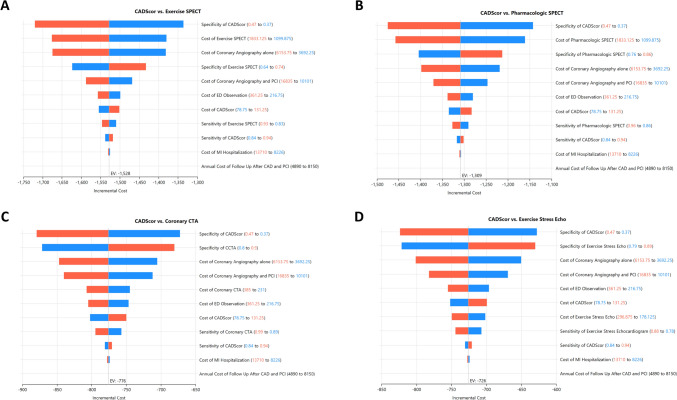
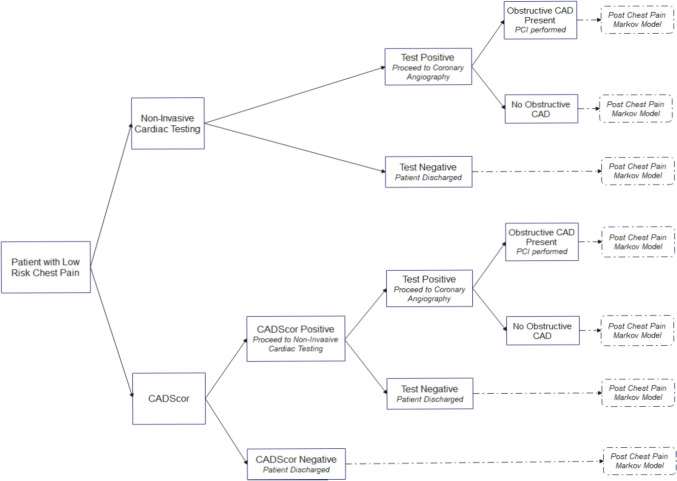
Methods: A two-part economic model, consisting of a decision analytic tree followed by a short-term Markov model, was developed to compare 1-year costs and outcomes (e.g., quality-adjusted life year [QALY], false-negatives, and related cardiac events) associated with the CADScor System as the first-line test versus other noninvasive cardiac tests from the perspective of the US healthcare system (TreeAge Pro). Model inputs were derived from literature, and costs for treatment strategies were calculated from average US reimbursements associated with Current Procedural Terminology and Medicare Severity Diagnosis Related Group codes. Values were reported in 2023 US dollars (USD). Parameter uncertainty was assessed through a series of deterministic and one-way sensitivity analyses.
Results: Base case results demonstrated that a CADScor-First strategy was cost saving compared with other noninvasive cardiac tests without a substantial difference in adverse events. Economic results were consistent when coronary artery disease (CAD) prevalence rates were varied from 2 to 30% and across a variety of sensitivity analyses. The overall cost savings were estimated to be $7.3-15.3 million USD per 10,000 patients with low-risk chest pain.
Conclusions: Use of a CADScor-First strategy in the evaluation of patients with low-risk chest pain presenting to the ED may result in substantial cost savings for the US healthcare system. More research is needed to understand the long-term costs and outcomes of this strategy.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


