Stefan W Koester, Brandon K Hoglund, Joelle N Hartke, Robert F Rudy, Ashutosh P Jadhav, Andrew F Ducruet, Felipe C Albuquerque, Joshua S Catapano, Laura A Snyder, Michael T Lawton
{"title":"动脉瘤性蛛网膜下腔出血后的抑郁:一种筛查工具和出院用户界面的开发。","authors":"Stefan W Koester, Brandon K Hoglund, Joelle N Hartke, Robert F Rudy, Ashutosh P Jadhav, Andrew F Ducruet, Felipe C Albuquerque, Joshua S Catapano, Laura A Snyder, Michael T Lawton","doi":"10.1007/s00701-025-06567-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A method for identification of chronic depression after aneurysmal subarachnoid hemorrhage (aSAH), risk stratification, and counseling is needed. This study aimed to develop a scoring system for post-aSAH depression and a user interface to supplement discharge counseling for patients.</p><p><strong>Methods: </strong>Based on a published prediction model for posttreatment depression risk among aSAH patients, a scale was developed using the beta coefficients of the final predictive model. The 5-point scale was based on 4 characteristics: tobacco use (2 points), chronic obstructive pulmonary disease (1 point), diabetes (1 point), and nonsaccular aneurysm type (1 point). A score of 1 was defined as low risk, a score of 2 or 3 was defined as medium risk, and a score of 4 or 5 was defined as high risk. The scale was then validated in a cohort of 514 patients treated at a single center. An interactive application was developed.</p><p><strong>Results: </strong>The rate of posttreatment depression among aSAH patients was 29.6% (152 of 514). The low-risk group had a nonsignificant increase in depression risk (relative risk [RR] [95% CI] = 0.89 [0.59-1.33], p = 0.71) compared with those with a score of 0. Significant increases in depression risk were found in the medium-risk (RR [95% CI] = 1.78 [1.34-2.37], p < 0.001) and high-risk (RR [95% CI] = 2.29 [1.28-4.09], p < 0.001) groups.</p><p><strong>Conclusions: </strong>A substantial percentage of patients in our cohort experienced major depressive disorder symptoms after aSAH treatment. An easy-to-use prediction and risk stratification tool for posttreatment depression among aSAH patients is available.</p>","PeriodicalId":7370,"journal":{"name":"Acta Neurochirurgica","volume":"167 1","pages":"176"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12187871/pdf/","citationCount":"0","resultStr":"{\"title\":\"Depression after aneurysmal subarachnoid hemorrhage: development of a screening tool and discharge user interface.\",\"authors\":\"Stefan W Koester, Brandon K Hoglund, Joelle N Hartke, Robert F Rudy, Ashutosh P Jadhav, Andrew F Ducruet, Felipe C Albuquerque, Joshua S Catapano, Laura A Snyder, Michael T Lawton\",\"doi\":\"10.1007/s00701-025-06567-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A method for identification of chronic depression after aneurysmal subarachnoid hemorrhage (aSAH), risk stratification, and counseling is needed. This study aimed to develop a scoring system for post-aSAH depression and a user interface to supplement discharge counseling for patients.</p><p><strong>Methods: </strong>Based on a published prediction model for posttreatment depression risk among aSAH patients, a scale was developed using the beta coefficients of the final predictive model. The 5-point scale was based on 4 characteristics: tobacco use (2 points), chronic obstructive pulmonary disease (1 point), diabetes (1 point), and nonsaccular aneurysm type (1 point). A score of 1 was defined as low risk, a score of 2 or 3 was defined as medium risk, and a score of 4 or 5 was defined as high risk. The scale was then validated in a cohort of 514 patients treated at a single center. An interactive application was developed.</p><p><strong>Results: </strong>The rate of posttreatment depression among aSAH patients was 29.6% (152 of 514). The low-risk group had a nonsignificant increase in depression risk (relative risk [RR] [95% CI] = 0.89 [0.59-1.33], p = 0.71) compared with those with a score of 0. Significant increases in depression risk were found in the medium-risk (RR [95% CI] = 1.78 [1.34-2.37], p < 0.001) and high-risk (RR [95% CI] = 2.29 [1.28-4.09], p < 0.001) groups.</p><p><strong>Conclusions: </strong>A substantial percentage of patients in our cohort experienced major depressive disorder symptoms after aSAH treatment. An easy-to-use prediction and risk stratification tool for posttreatment depression among aSAH patients is available.</p>\",\"PeriodicalId\":7370,\"journal\":{\"name\":\"Acta Neurochirurgica\",\"volume\":\"167 1\",\"pages\":\"176\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12187871/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Neurochirurgica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00701-025-06567-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Neurochirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00701-025-06567-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Depression after aneurysmal subarachnoid hemorrhage: development of a screening tool and discharge user interface.
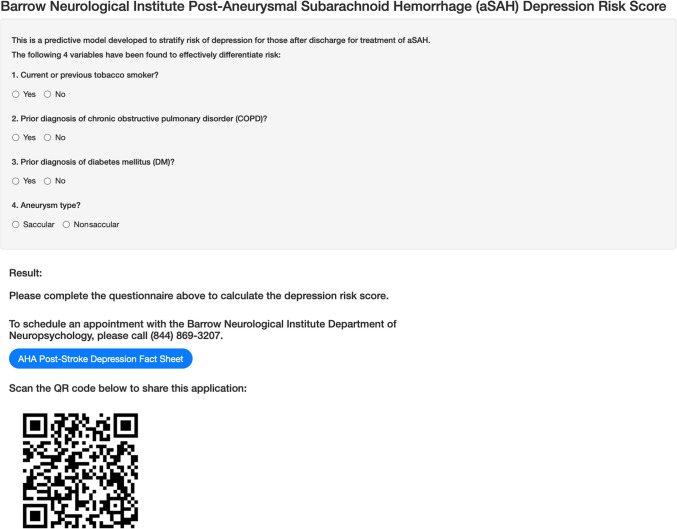
Background: A method for identification of chronic depression after aneurysmal subarachnoid hemorrhage (aSAH), risk stratification, and counseling is needed. This study aimed to develop a scoring system for post-aSAH depression and a user interface to supplement discharge counseling for patients.
Methods: Based on a published prediction model for posttreatment depression risk among aSAH patients, a scale was developed using the beta coefficients of the final predictive model. The 5-point scale was based on 4 characteristics: tobacco use (2 points), chronic obstructive pulmonary disease (1 point), diabetes (1 point), and nonsaccular aneurysm type (1 point). A score of 1 was defined as low risk, a score of 2 or 3 was defined as medium risk, and a score of 4 or 5 was defined as high risk. The scale was then validated in a cohort of 514 patients treated at a single center. An interactive application was developed.
Results: The rate of posttreatment depression among aSAH patients was 29.6% (152 of 514). The low-risk group had a nonsignificant increase in depression risk (relative risk [RR] [95% CI] = 0.89 [0.59-1.33], p = 0.71) compared with those with a score of 0. Significant increases in depression risk were found in the medium-risk (RR [95% CI] = 1.78 [1.34-2.37], p < 0.001) and high-risk (RR [95% CI] = 2.29 [1.28-4.09], p < 0.001) groups.
Conclusions: A substantial percentage of patients in our cohort experienced major depressive disorder symptoms after aSAH treatment. An easy-to-use prediction and risk stratification tool for posttreatment depression among aSAH patients is available.
期刊介绍:
The journal "Acta Neurochirurgica" publishes only original papers useful both to research and clinical work. Papers should deal with clinical neurosurgery - diagnosis and diagnostic techniques, operative surgery and results, postoperative treatment - or with research work in neuroscience if the underlying questions or the results are of neurosurgical interest. Reports on congresses are given in brief accounts. As official organ of the European Association of Neurosurgical Societies the journal publishes all announcements of the E.A.N.S. and reports on the activities of its member societies. Only contributions written in English will be accepted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


