Alexander Evans, Jill VanWyk, Margee Kerr, Amy Couper, Wilson D Pace, Yasir Tarabichi, Rachel Pullen, Michael Pollack, M Bradley Drummond, Jill Ohar, Catherine Meldrum, MeiLan K Han, Alan Kaplan, Tonya Winders, Juan Wisnivesky, Barry Make, Alex Federman, Victoria Carter, Katie Lang, Douglas Mapel, Nicola A Hanania, Daiana Stolz, Fernando J Martinez, David Price
{"title":"在美国实现系统变革的实用策略:来自CONQUEST质量改进计划的经验教训和见解。","authors":"Alexander Evans, Jill VanWyk, Margee Kerr, Amy Couper, Wilson D Pace, Yasir Tarabichi, Rachel Pullen, Michael Pollack, M Bradley Drummond, Jill Ohar, Catherine Meldrum, MeiLan K Han, Alan Kaplan, Tonya Winders, Juan Wisnivesky, Barry Make, Alex Federman, Victoria Carter, Katie Lang, Douglas Mapel, Nicola A Hanania, Daiana Stolz, Fernando J Martinez, David Price","doi":"10.1017/S1463423625100170","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Quality improvement programmes (QIPs) are designed to enhance patient outcomes by systematically introducing evidence-based clinical practices. The CONQUEST QIP focuses on improving the identification and management of patients with COPD in primary care. The process of developing CONQUEST, recruiting, preparing systems for participation, and implementing the QIP across three integrated healthcare systems (IHSs) is examined to identify and share lessons learned.</p><p><strong>Approach and development: </strong>This review is organized into three stages: 1) development, 2) preparing IHSs for implementation, and 3) implementation. In each stage, key steps are described with the lessons learned and how they can inform others interested in developing QIPs designed to improve the care of patients with chronic conditions in primary care.Stage 1 was establishing and working with steering committees to develop the QIP Quality Standards, define the target patient population, assess current management practices, and create a global operational protocol. Additionally, potential IHSs were assessed for feasibility of QIP integration into primary care practices. Factors assessed included a review of technological infrastructure, QI experience, and capacity for effective implementation.Stage 2 was preparation for implementation. Key was enlisting clinical champions to advocate for the QIP, secure participation in primary care, and establish effective communication channels. Preparation for implementation required obtaining IHS approvals, ensuring Health Insurance Portability and Accountability Act compliance, and devising operational strategies for patient outreach and clinical decision support delivery.Stage 3 was developing three IHS implementation models. With insight into the local context from local clinicians, implementation models were adapted to work with the resources and capacity of the IHSs while ensuring the delivery of essential elements of the programme.</p><p><strong>Conclusion: </strong>Developing and launching a QIP programme across primary care practices requires extensive groundwork, preparation, and committed local champions to assist in building an adaptable environment that encourages open communication and is receptive to feedback.</p>","PeriodicalId":74493,"journal":{"name":"Primary health care research & development","volume":"26 ","pages":"e50"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12188133/pdf/","citationCount":"0","resultStr":"{\"title\":\"Practical strategies for achieving system change in the US: lessons and insights from the CONQUEST quality improvement programme.\",\"authors\":\"Alexander Evans, Jill VanWyk, Margee Kerr, Amy Couper, Wilson D Pace, Yasir Tarabichi, Rachel Pullen, Michael Pollack, M Bradley Drummond, Jill Ohar, Catherine Meldrum, MeiLan K Han, Alan Kaplan, Tonya Winders, Juan Wisnivesky, Barry Make, Alex Federman, Victoria Carter, Katie Lang, Douglas Mapel, Nicola A Hanania, Daiana Stolz, Fernando J Martinez, David Price\",\"doi\":\"10.1017/S1463423625100170\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Quality improvement programmes (QIPs) are designed to enhance patient outcomes by systematically introducing evidence-based clinical practices. The CONQUEST QIP focuses on improving the identification and management of patients with COPD in primary care. The process of developing CONQUEST, recruiting, preparing systems for participation, and implementing the QIP across three integrated healthcare systems (IHSs) is examined to identify and share lessons learned.</p><p><strong>Approach and development: </strong>This review is organized into three stages: 1) development, 2) preparing IHSs for implementation, and 3) implementation. In each stage, key steps are described with the lessons learned and how they can inform others interested in developing QIPs designed to improve the care of patients with chronic conditions in primary care.Stage 1 was establishing and working with steering committees to develop the QIP Quality Standards, define the target patient population, assess current management practices, and create a global operational protocol. Additionally, potential IHSs were assessed for feasibility of QIP integration into primary care practices. Factors assessed included a review of technological infrastructure, QI experience, and capacity for effective implementation.Stage 2 was preparation for implementation. Key was enlisting clinical champions to advocate for the QIP, secure participation in primary care, and establish effective communication channels. Preparation for implementation required obtaining IHS approvals, ensuring Health Insurance Portability and Accountability Act compliance, and devising operational strategies for patient outreach and clinical decision support delivery.Stage 3 was developing three IHS implementation models. With insight into the local context from local clinicians, implementation models were adapted to work with the resources and capacity of the IHSs while ensuring the delivery of essential elements of the programme.</p><p><strong>Conclusion: </strong>Developing and launching a QIP programme across primary care practices requires extensive groundwork, preparation, and committed local champions to assist in building an adaptable environment that encourages open communication and is receptive to feedback.</p>\",\"PeriodicalId\":74493,\"journal\":{\"name\":\"Primary health care research & development\",\"volume\":\"26 \",\"pages\":\"e50\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-06-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12188133/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Primary health care research & development\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1017/S1463423625100170\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Primary health care research & development","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/S1463423625100170","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:质量改进计划(QIPs)旨在通过系统地引入循证临床实践来提高患者的治疗效果。CONQUEST QIP侧重于改善初级保健中COPD患者的识别和管理。研究了在三个综合医疗保健系统(ihs)中开发CONQUEST、招募、准备参与系统和实施QIP的过程,以确定和分享经验教训。方法和发展:本综述分为三个阶段:1)发展,2)准备实施ihs, 3)实施。在每个阶段中,都描述了关键步骤以及所吸取的经验教训,以及它们如何能够为其他有兴趣开发旨在改善初级保健中慢性病患者护理的QIPs的人提供信息。第一阶段是建立并与指导委员会合作,制定QIP质量标准,确定目标患者群体,评估当前的管理实践,并创建全球操作协议。此外,还评估了潜在的卫生服务提供者将质量保证ip纳入初级保健实践的可行性。评估的因素包括对技术基础设施、QI经验和有效实现能力的审查。第二阶段是准备实施。关键是争取临床倡导者倡导质量保证计划,确保参与初级保健,并建立有效的沟通渠道。实施的准备工作需要获得IHS的批准,确保《健康保险流通与责任法案》(Health Insurance Portability and Accountability Act)的合规,并为患者外展和提供临床决策支持制定业务战略。阶段3是开发三个IHS实现模型。根据当地临床医生对当地情况的了解,对实施模式进行了调整,以配合卫生保健机构的资源和能力,同时确保提供该规划的基本要素。结论:在初级保健实践中制定和启动QIP计划需要广泛的基础工作、准备工作和当地拥护者的承诺,以协助建立一个鼓励开放沟通和接受反馈的适应性环境。
Practical strategies for achieving system change in the US: lessons and insights from the CONQUEST quality improvement programme.
Background: Quality improvement programmes (QIPs) are designed to enhance patient outcomes by systematically introducing evidence-based clinical practices. The CONQUEST QIP focuses on improving the identification and management of patients with COPD in primary care. The process of developing CONQUEST, recruiting, preparing systems for participation, and implementing the QIP across three integrated healthcare systems (IHSs) is examined to identify and share lessons learned.
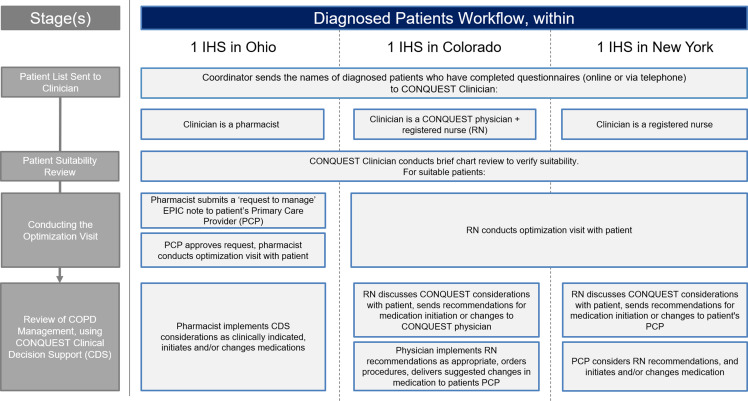
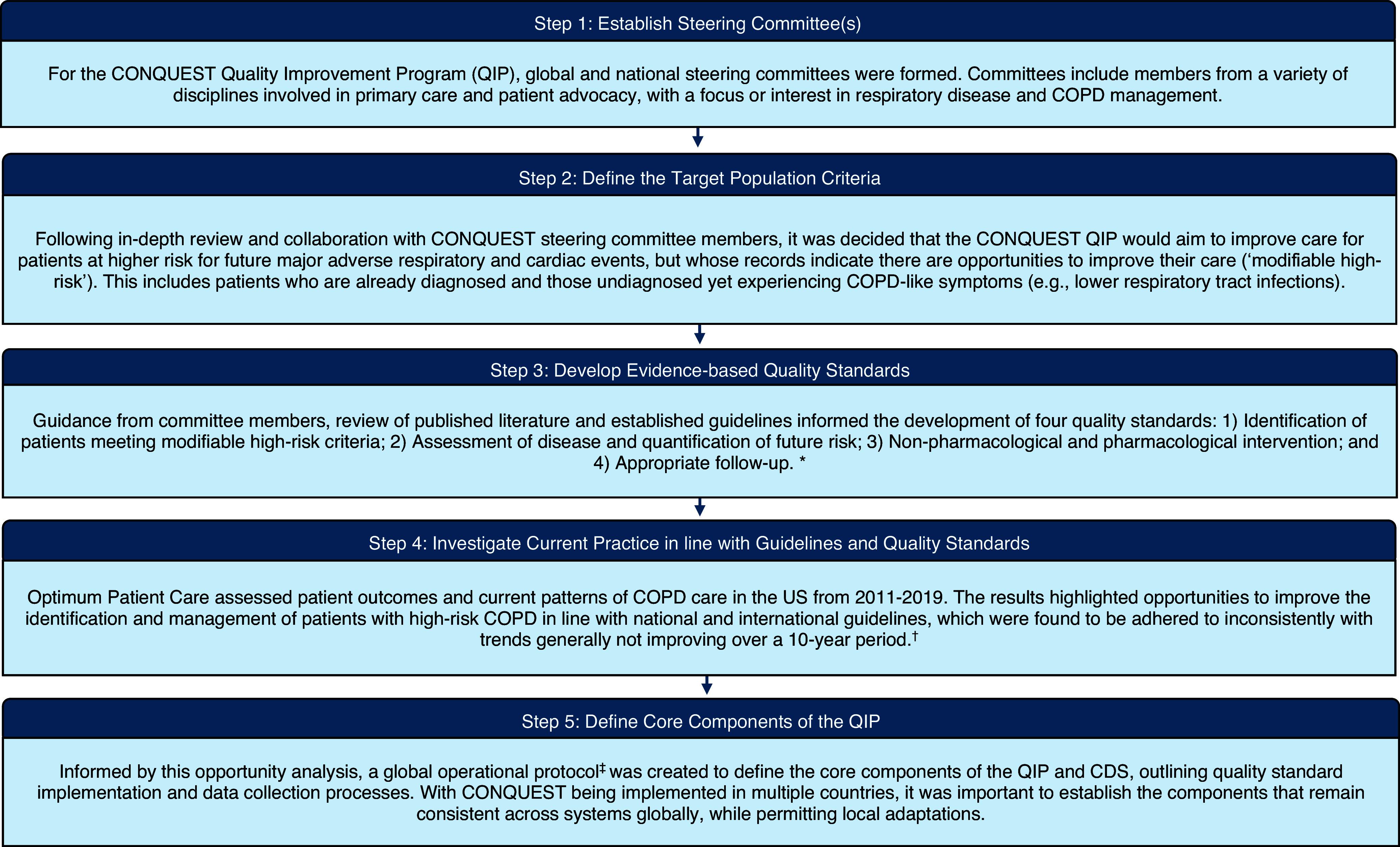
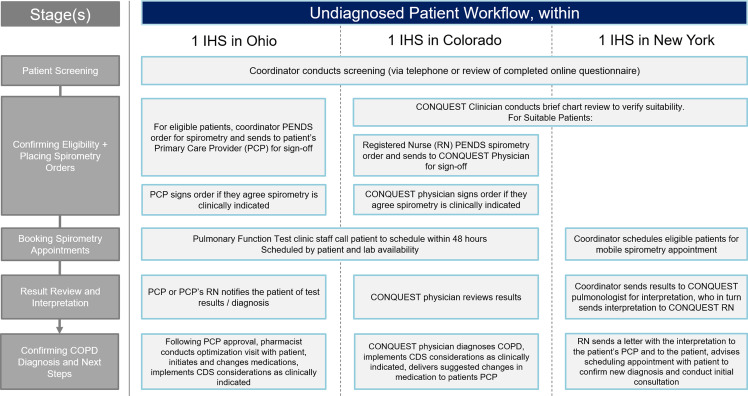
Approach and development: This review is organized into three stages: 1) development, 2) preparing IHSs for implementation, and 3) implementation. In each stage, key steps are described with the lessons learned and how they can inform others interested in developing QIPs designed to improve the care of patients with chronic conditions in primary care.Stage 1 was establishing and working with steering committees to develop the QIP Quality Standards, define the target patient population, assess current management practices, and create a global operational protocol. Additionally, potential IHSs were assessed for feasibility of QIP integration into primary care practices. Factors assessed included a review of technological infrastructure, QI experience, and capacity for effective implementation.Stage 2 was preparation for implementation. Key was enlisting clinical champions to advocate for the QIP, secure participation in primary care, and establish effective communication channels. Preparation for implementation required obtaining IHS approvals, ensuring Health Insurance Portability and Accountability Act compliance, and devising operational strategies for patient outreach and clinical decision support delivery.Stage 3 was developing three IHS implementation models. With insight into the local context from local clinicians, implementation models were adapted to work with the resources and capacity of the IHSs while ensuring the delivery of essential elements of the programme.
Conclusion: Developing and launching a QIP programme across primary care practices requires extensive groundwork, preparation, and committed local champions to assist in building an adaptable environment that encourages open communication and is receptive to feedback.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


