Mohammed Almubayyidh, David A Jenkins, Edoardo Gaude, Adrian R Parry-Jones
{"title":"整合临床预测因子和胶质纤维酸性蛋白在院前诊断疑似脑卒中脑出血预测模型中的应用。","authors":"Mohammed Almubayyidh, David A Jenkins, Edoardo Gaude, Adrian R Parry-Jones","doi":"10.1136/bmjno-2025-001160","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong></p><p><strong>Introduction: </strong>Accurate and timely differentiation of intracerebral haemorrhage (ICH) from other suspected stroke cases is crucial in prehospital settings, where early blood pressure reduction in the ambulance can improve outcomes. This study aims to assess whether combining clinical predictors and glial fibrillary acidic protein (GFAP) in prediction models can effectively distinguish ICH from other suspected stroke cases.</p><p><strong>Methods: </strong>Data were derived from the Testing for Identification Markers of Stroke trial, a prospective diagnostic accuracy study. Suspected stroke patients within 6 hours of symptom onset were included. Clinical predictors were selected based on known associations with ICH, and a predefined GFAP cut-off of 290 pg/mL was applied. Logistic regression was used to assess the performance of clinical predictors and GFAP, individually and in combination. Internal validation and optimism correction were performed via bootstrapping, and comparisons of the area under the curve (AUC) were conducted using DeLong's test.</p><p><strong>Results: </strong>We included 209 suspected stroke cases, of which 5% were finally diagnosed with ICH. Clinical predictors alone achieved an optimism-corrected AUC of 0.74 (95% CI 0.60 to 0.88), while GFAP alone resulted in an optimism-corrected AUC of 0.83 (95% CI 0.69 to 0.99). Combining clinical predictors with GFAP significantly enhanced the AUC, yielding an optimism-corrected value of 0.90 (95% CI 0.79 to 0.98). This combined model also demonstrated high predictive accuracy, with an optimism-corrected sensitivity of 60% (95% CI 29.0% to 90.0%) and a specificity of 98% (95% CI 96.1% to 100.0%).</p><p><strong>Conclusions: </strong>Combining clinical predictors with GFAP shows promise for the prehospital identification of ICH to support transport decision-making and potentially initiate treatment while en route for these patients. Prospective validation using portable point-of-care devices is required to confirm the utility of this approach in the prehospital setting.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"7 1","pages":"e001160"},"PeriodicalIF":2.4000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12182047/pdf/","citationCount":"0","resultStr":"{\"title\":\"Integrating clinical predictors and glial fibrillary acidic protein in prediction models for the prehospital identification of intracerebral haemorrhage in suspected stroke.\",\"authors\":\"Mohammed Almubayyidh, David A Jenkins, Edoardo Gaude, Adrian R Parry-Jones\",\"doi\":\"10.1136/bmjno-2025-001160\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong></p><p><strong>Introduction: </strong>Accurate and timely differentiation of intracerebral haemorrhage (ICH) from other suspected stroke cases is crucial in prehospital settings, where early blood pressure reduction in the ambulance can improve outcomes. This study aims to assess whether combining clinical predictors and glial fibrillary acidic protein (GFAP) in prediction models can effectively distinguish ICH from other suspected stroke cases.</p><p><strong>Methods: </strong>Data were derived from the Testing for Identification Markers of Stroke trial, a prospective diagnostic accuracy study. Suspected stroke patients within 6 hours of symptom onset were included. Clinical predictors were selected based on known associations with ICH, and a predefined GFAP cut-off of 290 pg/mL was applied. Logistic regression was used to assess the performance of clinical predictors and GFAP, individually and in combination. Internal validation and optimism correction were performed via bootstrapping, and comparisons of the area under the curve (AUC) were conducted using DeLong's test.</p><p><strong>Results: </strong>We included 209 suspected stroke cases, of which 5% were finally diagnosed with ICH. Clinical predictors alone achieved an optimism-corrected AUC of 0.74 (95% CI 0.60 to 0.88), while GFAP alone resulted in an optimism-corrected AUC of 0.83 (95% CI 0.69 to 0.99). Combining clinical predictors with GFAP significantly enhanced the AUC, yielding an optimism-corrected value of 0.90 (95% CI 0.79 to 0.98). This combined model also demonstrated high predictive accuracy, with an optimism-corrected sensitivity of 60% (95% CI 29.0% to 90.0%) and a specificity of 98% (95% CI 96.1% to 100.0%).</p><p><strong>Conclusions: </strong>Combining clinical predictors with GFAP shows promise for the prehospital identification of ICH to support transport decision-making and potentially initiate treatment while en route for these patients. Prospective validation using portable point-of-care devices is required to confirm the utility of this approach in the prehospital setting.</p>\",\"PeriodicalId\":52754,\"journal\":{\"name\":\"BMJ Neurology Open\",\"volume\":\"7 1\",\"pages\":\"e001160\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12182047/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Neurology Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjno-2025-001160\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2025-001160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
摘要:引言:准确和及时地区分脑出血(ICH)与其他疑似中风病例在院前环境中至关重要,在救护车中早期降低血压可以改善预后。本研究旨在评估在预测模型中结合临床预测因子和胶质纤维酸性蛋白(GFAP)是否能有效区分脑出血与其他疑似脑卒中病例。方法:数据来源于卒中识别标记物测试试验,这是一项前瞻性诊断准确性研究。纳入症状出现6小时内的疑似脑卒中患者。根据已知的与脑出血的关联选择临床预测因子,并采用预定义的GFAP临界值290 pg/mL。采用Logistic回归单独或联合评估临床预测指标和GFAP的表现。采用bootstrapping进行内部验证和乐观校正,采用DeLong’s test比较曲线下面积(AUC)。结果:我们纳入了209例疑似脑卒中病例,其中5%最终诊断为脑出血。单独的临床预测获得了0.74的乐观校正AUC (95% CI 0.60 - 0.88),而单独的GFAP导致了0.83的乐观校正AUC (95% CI 0.69 - 0.99)。结合临床预测因子和GFAP显著提高了AUC,得到了0.90的乐观校正值(95% CI 0.79 - 0.98)。该联合模型也显示出较高的预测准确性,乐观校正后的灵敏度为60% (95% CI 29.0%至90.0%),特异性为98% (95% CI 96.1%至100.0%)。结论:将临床预测指标与GFAP相结合,有望在院前识别脑出血,以支持转运决策,并可能在途中为这些患者启动治疗。需要使用便携式护理点设备进行前瞻性验证,以确认该方法在院前环境中的实用性。
Integrating clinical predictors and glial fibrillary acidic protein in prediction models for the prehospital identification of intracerebral haemorrhage in suspected stroke.
Abstract:
Introduction: Accurate and timely differentiation of intracerebral haemorrhage (ICH) from other suspected stroke cases is crucial in prehospital settings, where early blood pressure reduction in the ambulance can improve outcomes. This study aims to assess whether combining clinical predictors and glial fibrillary acidic protein (GFAP) in prediction models can effectively distinguish ICH from other suspected stroke cases.
Methods: Data were derived from the Testing for Identification Markers of Stroke trial, a prospective diagnostic accuracy study. Suspected stroke patients within 6 hours of symptom onset were included. Clinical predictors were selected based on known associations with ICH, and a predefined GFAP cut-off of 290 pg/mL was applied. Logistic regression was used to assess the performance of clinical predictors and GFAP, individually and in combination. Internal validation and optimism correction were performed via bootstrapping, and comparisons of the area under the curve (AUC) were conducted using DeLong's test.
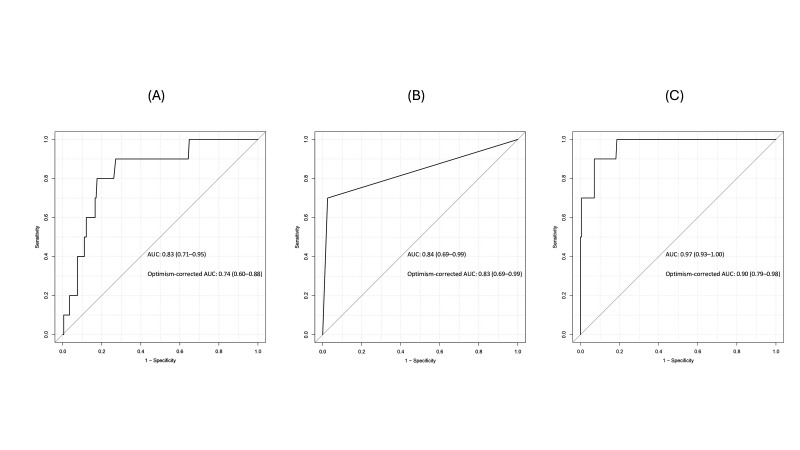
Results: We included 209 suspected stroke cases, of which 5% were finally diagnosed with ICH. Clinical predictors alone achieved an optimism-corrected AUC of 0.74 (95% CI 0.60 to 0.88), while GFAP alone resulted in an optimism-corrected AUC of 0.83 (95% CI 0.69 to 0.99). Combining clinical predictors with GFAP significantly enhanced the AUC, yielding an optimism-corrected value of 0.90 (95% CI 0.79 to 0.98). This combined model also demonstrated high predictive accuracy, with an optimism-corrected sensitivity of 60% (95% CI 29.0% to 90.0%) and a specificity of 98% (95% CI 96.1% to 100.0%).
Conclusions: Combining clinical predictors with GFAP shows promise for the prehospital identification of ICH to support transport decision-making and potentially initiate treatment while en route for these patients. Prospective validation using portable point-of-care devices is required to confirm the utility of this approach in the prehospital setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


