{"title":"龟头复发性脓疱病变的难题。","authors":"Febin Ashraf, Jayashankar Errukkambattu","doi":"10.4103/ijstd.ijstd_41_25","DOIUrl":null,"url":null,"abstract":"<p><p>Genital psoriasis rarely presents as isolated pustular lesions confined to the glans penis, often leading to misdiagnosis as sexually transmitted infections such as herpes genitalis. We report a 36-year-old male with recurrent pruritic lesions on the glans over four months, with seasonal exacerbations over the past three years, particularly in winter and summer. The patient, with no systemic comorbidities or extragenital lesions, was initially misdiagnosed and treated with antivirals without relief. Clinical examination revealed multiple erythematous papules with collarette of scale and pustules that ruptured to form non-scarring erosions. Histopathological examination confirmed pustular psoriasis. The patient responded completely to topical 2% tofacitinib within four weeks. Isolated genital pustular psoriasis is exceedingly rare, with limited cases reported in the literature. Diagnostic delay is common due to its overlap with other genital dermatoses and lack of typical psoriatic plaques. This case highlights the importance of considering non-venereal causes in persistent genital lesions and the role of histopathology in achieving accurate diagnosis.</p>","PeriodicalId":44880,"journal":{"name":"Indian Journal of Sexually Transmitted Diseases and AIDS","volume":"46 1","pages":"71-73"},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12180853/pdf/","citationCount":"0","resultStr":"{\"title\":\"A conundrum of recurrent pustular lesions of the glans.\",\"authors\":\"Febin Ashraf, Jayashankar Errukkambattu\",\"doi\":\"10.4103/ijstd.ijstd_41_25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Genital psoriasis rarely presents as isolated pustular lesions confined to the glans penis, often leading to misdiagnosis as sexually transmitted infections such as herpes genitalis. We report a 36-year-old male with recurrent pruritic lesions on the glans over four months, with seasonal exacerbations over the past three years, particularly in winter and summer. The patient, with no systemic comorbidities or extragenital lesions, was initially misdiagnosed and treated with antivirals without relief. Clinical examination revealed multiple erythematous papules with collarette of scale and pustules that ruptured to form non-scarring erosions. Histopathological examination confirmed pustular psoriasis. The patient responded completely to topical 2% tofacitinib within four weeks. Isolated genital pustular psoriasis is exceedingly rare, with limited cases reported in the literature. Diagnostic delay is common due to its overlap with other genital dermatoses and lack of typical psoriatic plaques. This case highlights the importance of considering non-venereal causes in persistent genital lesions and the role of histopathology in achieving accurate diagnosis.</p>\",\"PeriodicalId\":44880,\"journal\":{\"name\":\"Indian Journal of Sexually Transmitted Diseases and AIDS\",\"volume\":\"46 1\",\"pages\":\"71-73\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12180853/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Journal of Sexually Transmitted Diseases and AIDS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ijstd.ijstd_41_25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Sexually Transmitted Diseases and AIDS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijstd.ijstd_41_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/9 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
A conundrum of recurrent pustular lesions of the glans.
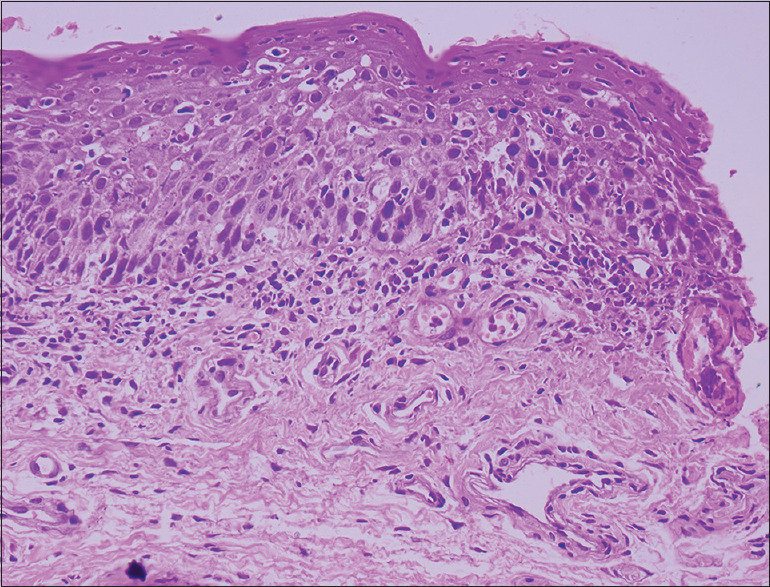
Genital psoriasis rarely presents as isolated pustular lesions confined to the glans penis, often leading to misdiagnosis as sexually transmitted infections such as herpes genitalis. We report a 36-year-old male with recurrent pruritic lesions on the glans over four months, with seasonal exacerbations over the past three years, particularly in winter and summer. The patient, with no systemic comorbidities or extragenital lesions, was initially misdiagnosed and treated with antivirals without relief. Clinical examination revealed multiple erythematous papules with collarette of scale and pustules that ruptured to form non-scarring erosions. Histopathological examination confirmed pustular psoriasis. The patient responded completely to topical 2% tofacitinib within four weeks. Isolated genital pustular psoriasis is exceedingly rare, with limited cases reported in the literature. Diagnostic delay is common due to its overlap with other genital dermatoses and lack of typical psoriatic plaques. This case highlights the importance of considering non-venereal causes in persistent genital lesions and the role of histopathology in achieving accurate diagnosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


