Andreas F Dalen, Martin G Gregersen, Aleksander L Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A Nilsen, Marius Molund
{"title":"腓骨钢板固定和胫后深韧带修复对三角韧带完全切片Weber B骨折模型踝关节稳定性的影响。","authors":"Andreas F Dalen, Martin G Gregersen, Aleksander L Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A Nilsen, Marius Molund","doi":"10.1177/10711007251334085","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.</p><p><strong>Methods: </strong>We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.</p><p><strong>Results: </strong>When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, <i>P</i> ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, <i>P</i> ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, <i>P</i> ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI -0.07 to 0.54, <i>P</i> = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, <i>P</i> = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, <i>P</i> ≤ .001).</p><p><strong>Conclusion: </strong>This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.</p><p><strong>Clinical relevance: </strong>Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.</p>","PeriodicalId":94011,"journal":{"name":"Foot & ankle international","volume":" ","pages":"688-696"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227801/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning.\",\"authors\":\"Andreas F Dalen, Martin G Gregersen, Aleksander L Skrede, Øystein Bjelland, Alf Inge Hellevik, Tor Åge Myklebust, Fredrik A Nilsen, Marius Molund\",\"doi\":\"10.1177/10711007251334085\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.</p><p><strong>Methods: </strong>We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.</p><p><strong>Results: </strong>When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, <i>P</i> ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, <i>P</i> ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, <i>P</i> ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI -0.07 to 0.54, <i>P</i> = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, <i>P</i> = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, <i>P</i> ≤ .001).</p><p><strong>Conclusion: </strong>This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.</p><p><strong>Clinical relevance: </strong>Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.</p>\",\"PeriodicalId\":94011,\"journal\":{\"name\":\"Foot & ankle international\",\"volume\":\" \",\"pages\":\"688-696\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227801/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Foot & ankle international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/10711007251334085\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & ankle international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/10711007251334085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:Weber B(旋后外旋)踝关节骨折伴完全性三角韧带断裂(SER4b)通常被认为是不稳定的,采用腓骨钢板固定治疗。最近的研究表明,深胫后韧带(dPTTL)具有重要的踝关节稳定作用,这对目前的实践提出了质疑。据我们所知,关于钢板固定的生物力学效应的研究很少,关于dPTTL修复的研究也没有。因此,本研究旨在评估腓骨钢板固定和dPTTL修复对完全性三角韧带切片Weber B骨折模型踝关节稳定性的影响。方法:对15具尸体踝关节标本进行5种状态的机器人测试:天然关节、SER4b损伤模型、SER4b钢板固定腓骨损伤模型、SER4b钢板固定修复模型、SER4b钢板固定与dPTTL联合修复模型。该机器人测量了踝关节的侧向平移、外翻和内外旋转的稳定性。在榫槽透视片上测量距骨移位和距骨倾斜。主要结果是中立踝关节位距位移的差异。结果:将钢板固定的SER4b损伤模型与踝关节进行比较,我们发现距骨移位的平均差异为1.18 mm (95% CI 0.88-1.48, P≤0.001),距骨倾斜的平均差异为14.47°(95% CI 12.90-16.05, P≤0.001),外旋的平均差异为11.44°(95% CI 9.00-13.87, P≤0.001)。将钢板固定和dPTTL联合修复的SER4b损伤模型与踝关节进行比较,我们发现距骨移位的平均差异为0.23 mm (95% CI为-0.07 ~ 0.54,P = 0.132),距骨倾斜的平均差异为1.65°(95% CI为0.07 ~ 3.22,P = 0.040),外旋的平均差异为5.26°(95% CI为2.82 ~ 7.70,P≤0.001)。结论:本研究的主要发现是在SER4b损伤模型中,仅腓骨钢板固定并不能显著提高踝关节稳定性。然而,当钢板固定和dPTTL修复相结合时,踝关节稳定性得到了显著改善。临床意义:我们的研究表明,除了钢板固定外,dPTTL修复可以改善Weber B SER4b骨折模型的踝关节稳定性。这些信息应该在未来的临床研究和治疗策略中加以考虑。
Effects of Fibular Plate Fixation and Deep Posterior Tibiotalar Ligament Repair on Ankle Stability in a Weber B Fracture Model with Complete Deltoid Ligament Sectioning.
Background: Weber B (supination external rotation) ankle fractures with complete deltoid ligament rupture (SER4b) are typically considered unstable and treated with plate fixation of the fibula. Recent studies have suggested a significant ankle-stabilizing role of the deep posterior tibiotalar ligament (dPTTL), which questions current practice. To our knowledge, there are few studies on the biomechanical effects of plate fixation and none on dPTTL repair. Therefore, this study aims to evaluate the effects of fibular plate fixation and dPTTL repair on ankle stability in a Weber B fracture model with complete deltoid ligament sectioning.
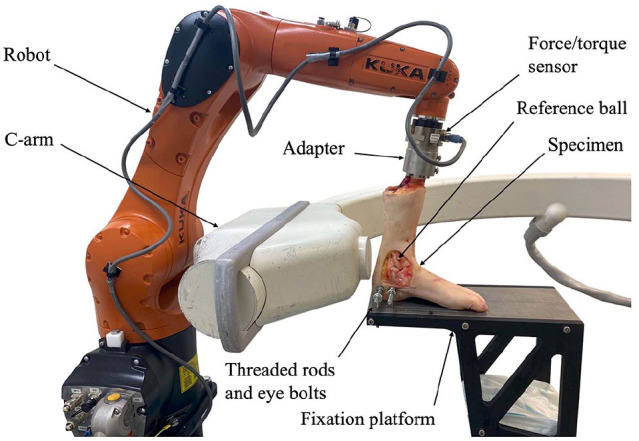
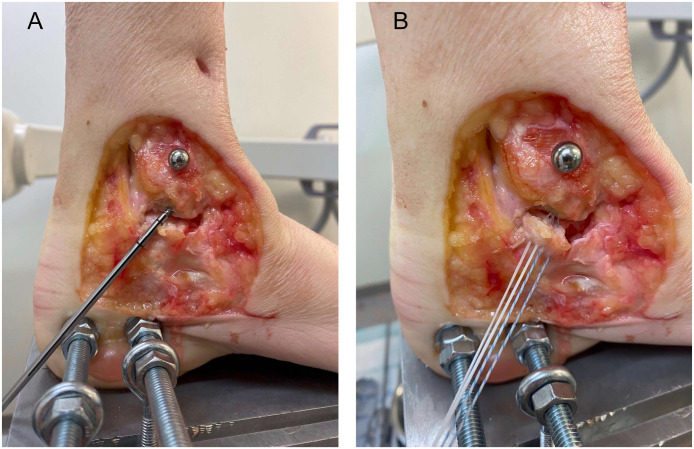
Methods: We robotically tested 15 cadaveric ankle specimens in 5 states: native joint, SER4b injury models, SER4b injury models with plate fixation of the fibula, SER4b injury models with dPTTL repair, and SER4b injury models with combined plate fixation and dPTTL repair. The robot measured ankle stability in lateral translation, valgus, and internal and external rotation. Talar shift and talar tilt were measured on mortise view radiographs. The primary outcome was differences in talar shift in neutral ankle position.
Results: When comparing SER4b injury models with plate fixation to native ankles, we found a mean difference in talar shift of 1.18 mm (95% CI 0.88-1.48, P ≤ .001), talar tilt of 14.47 degrees (95% CI 12.90-16.05, P ≤ .001), and external rotation of 11.44 degrees (95% CI 9.00-13.87, P ≤ .001). When comparing SER4b injury models with combined plate fixation and dPTTL repair to native ankles, we found a mean difference in talar shift of 0.23 mm (95% CI -0.07 to 0.54, P = .132), talar tilt of 1.65 degrees (95% CI 0.07-3.22, P = .040), and external rotation of 5.26 degrees (95% CI 2.82-7.70, P ≤ .001).
Conclusion: This study's main finding was that plate fixation of the fibula alone did not considerably enhance ankle stability in SER4b injury models. However, ankle stability was substantially improved when plate fixation and dPTTL repair were combined.
Clinical relevance: Our study showed that dPTTL repair, in addition to plate fixation, improved ankle stability in Weber B SER4b fracture models. This information should be considered in future clinical research and treatment strategies for these fractures.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


