{"title":"潜在急性冠脉综合征患者的主治医师和住院急诊医师的心脏评分一致性","authors":"Joel C Mosley, Greggory R Davis, Michael H Truax","doi":"10.31486/toj.24.0108","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chest pain in the emergency department requires swift diagnosis to distinguish between acute coronary syndrome and noncardiac causes. The use of the HEART score, which risk-stratifies patients based on history, electrocardiogram, age, risk factors, and troponin, reduces unnecessary admissions and costs. However, evaluations by resident physicians supervised by attending physicians can delay treatment and increase costs.</p><p><strong>Methods: </strong>We assessed interrater reliability between attending physician and resident physician HEART scores in 2 study phases. In phase 1, participants were not provided with a standardized form, but in phase 2, participants used a standardized form to calculate HEART scores. Differences in scores were compared by years of experience and by study phase.</p><p><strong>Results: </strong>A total of 75 HEART score comparisons were analyzed. Fifty comparisons between attending physicians and resident physicians were completed in phase 1, and 25 comparisons were completed in phase 2. Discrepancies between attending and resident physician scores ≤3 vs >3 decreased from 24% in phase 1 to 8% in phase 2. Attending physician years of experience did not affect discrepancies in HEART scores ≤3 vs >3 between attending and resident physicians (odds ratio [OR] 1.18 [95% CI 0.78 to 1.81]). Similarly, resident physician years of experience did not affect differences in HEART scores ≤3 vs >3 between attending and resident physicians (OR 0.77 [95% CI 0.38 to 1.53]).</p><p><strong>Conclusion: </strong>The study found good agreement between attending physician and resident physician HEART scores, with experience level not significantly affecting discrepancies. The standardized scoring form improved consistency, although not significantly.</p>","PeriodicalId":47600,"journal":{"name":"Ochsner Journal","volume":"25 2","pages":"77-84"},"PeriodicalIF":1.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12175770/pdf/","citationCount":"0","resultStr":"{\"title\":\"HEART Score Agreement Between Attending and Resident Emergency Medicine Physicians for Patients With Potential Acute Coronary Syndrome.\",\"authors\":\"Joel C Mosley, Greggory R Davis, Michael H Truax\",\"doi\":\"10.31486/toj.24.0108\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chest pain in the emergency department requires swift diagnosis to distinguish between acute coronary syndrome and noncardiac causes. The use of the HEART score, which risk-stratifies patients based on history, electrocardiogram, age, risk factors, and troponin, reduces unnecessary admissions and costs. However, evaluations by resident physicians supervised by attending physicians can delay treatment and increase costs.</p><p><strong>Methods: </strong>We assessed interrater reliability between attending physician and resident physician HEART scores in 2 study phases. In phase 1, participants were not provided with a standardized form, but in phase 2, participants used a standardized form to calculate HEART scores. Differences in scores were compared by years of experience and by study phase.</p><p><strong>Results: </strong>A total of 75 HEART score comparisons were analyzed. Fifty comparisons between attending physicians and resident physicians were completed in phase 1, and 25 comparisons were completed in phase 2. Discrepancies between attending and resident physician scores ≤3 vs >3 decreased from 24% in phase 1 to 8% in phase 2. Attending physician years of experience did not affect discrepancies in HEART scores ≤3 vs >3 between attending and resident physicians (odds ratio [OR] 1.18 [95% CI 0.78 to 1.81]). Similarly, resident physician years of experience did not affect differences in HEART scores ≤3 vs >3 between attending and resident physicians (OR 0.77 [95% CI 0.38 to 1.53]).</p><p><strong>Conclusion: </strong>The study found good agreement between attending physician and resident physician HEART scores, with experience level not significantly affecting discrepancies. The standardized scoring form improved consistency, although not significantly.</p>\",\"PeriodicalId\":47600,\"journal\":{\"name\":\"Ochsner Journal\",\"volume\":\"25 2\",\"pages\":\"77-84\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12175770/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ochsner Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31486/toj.24.0108\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ochsner Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31486/toj.24.0108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:胸痛在急诊科需要迅速诊断,以区分急性冠状动脉综合征和非心脏原因。使用HEART评分,根据病史、心电图、年龄、危险因素和肌钙蛋白对患者进行风险分层,减少了不必要的入院和费用。然而,住院医师在主治医师的监督下进行的评估可能会延误治疗并增加费用。方法:我们在2个研究阶段评估了主治医师和住院医师心脏评分之间的互译信度。在第一阶段,没有为参与者提供标准化表格,但在第二阶段,参与者使用标准化表格来计算HEART分数。分数的差异是根据经历的年限和学习的阶段来比较的。结果:共分析75例HEART评分比较。第一阶段完成了主治医生和住院医生之间的50项比较,第二阶段完成了25项比较。主治医师和住院医师评分≤3分与>.3分之间的差异从第一阶段的24%下降到第二阶段的8%。主治医师的工作年限不影响主治医师和住院医师在HEART评分≤3分和bb0.3分上的差异(优势比[OR] 1.18 [95% CI 0.78 ~ 1.81])。同样,住院医师的经验年数不影响主治医师和住院医师在心脏评分≤3分和bb0.3分上的差异(OR 0.77 [95% CI 0.38 ~ 1.53])。结论:研究发现主治医师和住院医师的心脏评分有很好的一致性,经验水平对差异没有显著影响。标准化计分表提高了一致性,尽管不是很明显。
HEART Score Agreement Between Attending and Resident Emergency Medicine Physicians for Patients With Potential Acute Coronary Syndrome.
Background: Chest pain in the emergency department requires swift diagnosis to distinguish between acute coronary syndrome and noncardiac causes. The use of the HEART score, which risk-stratifies patients based on history, electrocardiogram, age, risk factors, and troponin, reduces unnecessary admissions and costs. However, evaluations by resident physicians supervised by attending physicians can delay treatment and increase costs.
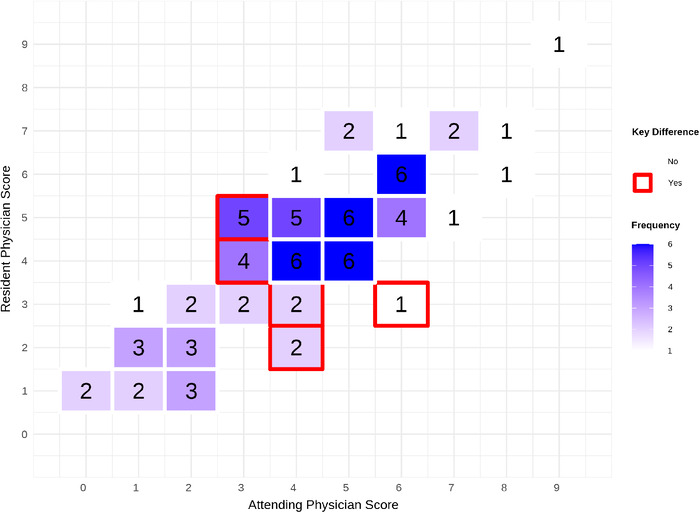
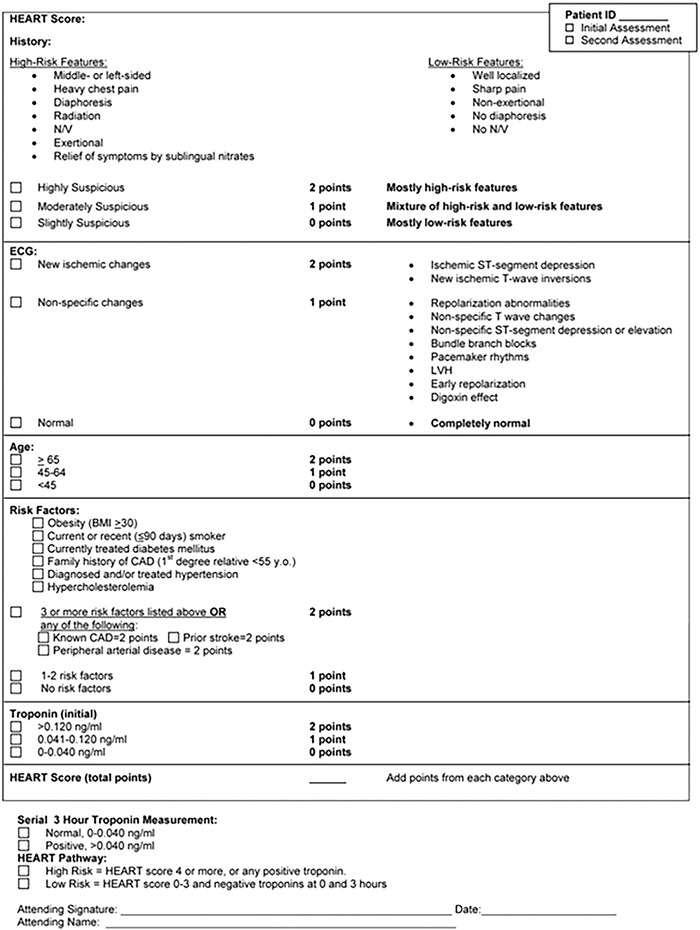
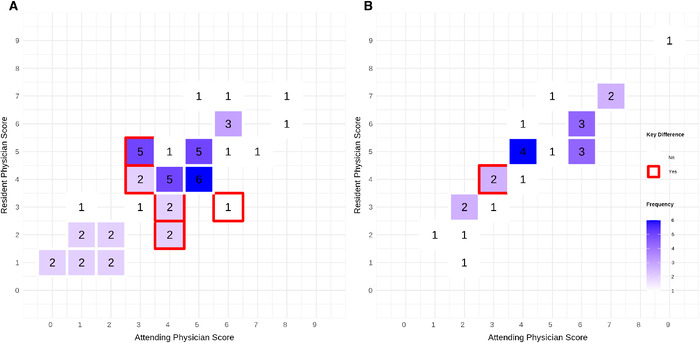
Methods: We assessed interrater reliability between attending physician and resident physician HEART scores in 2 study phases. In phase 1, participants were not provided with a standardized form, but in phase 2, participants used a standardized form to calculate HEART scores. Differences in scores were compared by years of experience and by study phase.
Results: A total of 75 HEART score comparisons were analyzed. Fifty comparisons between attending physicians and resident physicians were completed in phase 1, and 25 comparisons were completed in phase 2. Discrepancies between attending and resident physician scores ≤3 vs >3 decreased from 24% in phase 1 to 8% in phase 2. Attending physician years of experience did not affect discrepancies in HEART scores ≤3 vs >3 between attending and resident physicians (odds ratio [OR] 1.18 [95% CI 0.78 to 1.81]). Similarly, resident physician years of experience did not affect differences in HEART scores ≤3 vs >3 between attending and resident physicians (OR 0.77 [95% CI 0.38 to 1.53]).
Conclusion: The study found good agreement between attending physician and resident physician HEART scores, with experience level not significantly affecting discrepancies. The standardized scoring form improved consistency, although not significantly.
期刊介绍:
The Ochsner Journal is a quarterly publication designed to support Ochsner"s mission to improve the health of our community through a commitment to innovation in healthcare, medical research, and education. The Ochsner Journal provides an active dialogue on practice standards in today"s changing healthcare environment. Emphasis will be given to topics of great societal and medical significance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


