Shyamal Patel, Lucy Rose Howroyd, Helen Bucknall, Hussain Memon, Robert Morgan, Joo-Young Chun
{"title":"支气管和非支气管全身动脉栓塞治疗咯血的长期结果- 20年的经验。","authors":"Shyamal Patel, Lucy Rose Howroyd, Helen Bucknall, Hussain Memon, Robert Morgan, Joo-Young Chun","doi":"10.1186/s42155-025-00551-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bronchial artery embolisation (BAE) is considered the most effective non-surgical technique for management of moderate-massive haemoptysis. Associated risks include neurological compromise such as stroke and spinal cord ischaemia. We aim to evaluate post-procedural outcomes and complication rates.</p><p><strong>Materials and methods: </strong>A single-centre retrospective observational study was conducted for BAE cases performed between January 2002-June 2022 in a London teaching hospital. Data was collected from electronic medical records and Picture Archiving Communications System (PACS). Primary outcomes were measured, and statistical analysis was performed to identify risk factors for haemoptysis recurrence.</p><p><strong>Results: </strong>One hundred eleven patients underwent 141 procedures with technical success achieved in 87.8% and clinical success in 84.8%. The most common causes of haemoptysis were aspergilloma (24.8%), bronchiectasis (19.1%) and malignancy (11.3%). Haemoptysis recurrence occurred in 65 cases (46%) with 20 patients undergoing repeat embolisation. Aspergillosis, cystic fibrosis, and non-tuberculous pneumonia were identified as risk factors for recurrent haemoptysis (p < 0.005). Pre-procedure MDCTA did not improve technical success. The rate of stroke in the cohort was 6.4% (9 cases), which is more so than quoted in the literature. Four of these patients presented with apical cavitations secondary to infection (aspergilloma or bacterial pneumonia).</p><p><strong>Conclusions: </strong>BAE is an effective endovascular treatment in patients with massive and recurrent haemoptysis. However, there is a well-documented risk of recurrent symptoms and early mortality, particularly in the setting of aspergilloma, cystic fibrosis and non-tuberculous pneumonia. The risk of stroke should not be underestimated. Patients should be counselled appropriately during informed consent prior to embarking on BAE.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"51"},"PeriodicalIF":1.5000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12176713/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long term outcomes following embolisation of bronchial and non-bronchial systemic arteries for the management of haemoptysis - a 20-year experience.\",\"authors\":\"Shyamal Patel, Lucy Rose Howroyd, Helen Bucknall, Hussain Memon, Robert Morgan, Joo-Young Chun\",\"doi\":\"10.1186/s42155-025-00551-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Bronchial artery embolisation (BAE) is considered the most effective non-surgical technique for management of moderate-massive haemoptysis. Associated risks include neurological compromise such as stroke and spinal cord ischaemia. We aim to evaluate post-procedural outcomes and complication rates.</p><p><strong>Materials and methods: </strong>A single-centre retrospective observational study was conducted for BAE cases performed between January 2002-June 2022 in a London teaching hospital. Data was collected from electronic medical records and Picture Archiving Communications System (PACS). Primary outcomes were measured, and statistical analysis was performed to identify risk factors for haemoptysis recurrence.</p><p><strong>Results: </strong>One hundred eleven patients underwent 141 procedures with technical success achieved in 87.8% and clinical success in 84.8%. The most common causes of haemoptysis were aspergilloma (24.8%), bronchiectasis (19.1%) and malignancy (11.3%). Haemoptysis recurrence occurred in 65 cases (46%) with 20 patients undergoing repeat embolisation. Aspergillosis, cystic fibrosis, and non-tuberculous pneumonia were identified as risk factors for recurrent haemoptysis (p < 0.005). Pre-procedure MDCTA did not improve technical success. The rate of stroke in the cohort was 6.4% (9 cases), which is more so than quoted in the literature. Four of these patients presented with apical cavitations secondary to infection (aspergilloma or bacterial pneumonia).</p><p><strong>Conclusions: </strong>BAE is an effective endovascular treatment in patients with massive and recurrent haemoptysis. However, there is a well-documented risk of recurrent symptoms and early mortality, particularly in the setting of aspergilloma, cystic fibrosis and non-tuberculous pneumonia. The risk of stroke should not be underestimated. Patients should be counselled appropriately during informed consent prior to embarking on BAE.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":\"8 1\",\"pages\":\"51\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12176713/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-025-00551-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-025-00551-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Long term outcomes following embolisation of bronchial and non-bronchial systemic arteries for the management of haemoptysis - a 20-year experience.
Background: Bronchial artery embolisation (BAE) is considered the most effective non-surgical technique for management of moderate-massive haemoptysis. Associated risks include neurological compromise such as stroke and spinal cord ischaemia. We aim to evaluate post-procedural outcomes and complication rates.
Materials and methods: A single-centre retrospective observational study was conducted for BAE cases performed between January 2002-June 2022 in a London teaching hospital. Data was collected from electronic medical records and Picture Archiving Communications System (PACS). Primary outcomes were measured, and statistical analysis was performed to identify risk factors for haemoptysis recurrence.
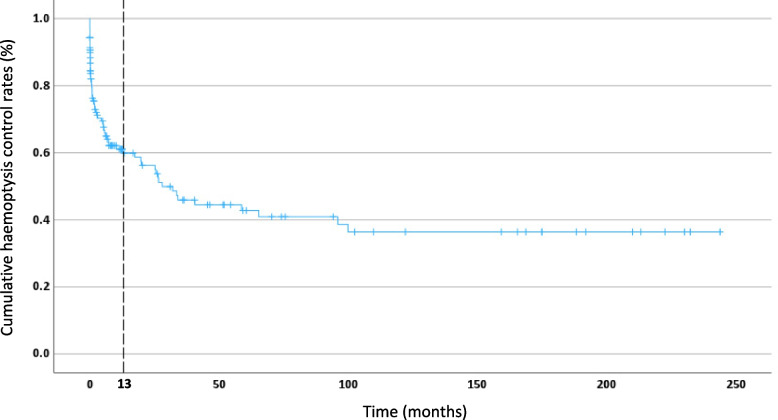
Results: One hundred eleven patients underwent 141 procedures with technical success achieved in 87.8% and clinical success in 84.8%. The most common causes of haemoptysis were aspergilloma (24.8%), bronchiectasis (19.1%) and malignancy (11.3%). Haemoptysis recurrence occurred in 65 cases (46%) with 20 patients undergoing repeat embolisation. Aspergillosis, cystic fibrosis, and non-tuberculous pneumonia were identified as risk factors for recurrent haemoptysis (p < 0.005). Pre-procedure MDCTA did not improve technical success. The rate of stroke in the cohort was 6.4% (9 cases), which is more so than quoted in the literature. Four of these patients presented with apical cavitations secondary to infection (aspergilloma or bacterial pneumonia).
Conclusions: BAE is an effective endovascular treatment in patients with massive and recurrent haemoptysis. However, there is a well-documented risk of recurrent symptoms and early mortality, particularly in the setting of aspergilloma, cystic fibrosis and non-tuberculous pneumonia. The risk of stroke should not be underestimated. Patients should be counselled appropriately during informed consent prior to embarking on BAE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


