{"title":"评价延长生命治疗成本-效果的相对生存模型:他法非地治疗转甲状腺素淀粉样变合并心肌病的应用。","authors":"Robert Young, Jack Said, Sam Large","doi":"10.1177/0272989X251342459","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundEconomic evaluations for life-extending treatments frequently require clinical trial data to be extrapolated beyond the trial duration to estimate changes in life expectancy. Conventional survival models often display hazard profiles that do not rise as expected in an aging population and require the incorporation of external data to ensure plausibility. Relative survival (RS) models can enable the incorporation of external data at model fitting. A comparison was performed between RS and \"standard\" all-cause survival (ACS) in modeling outcomes from the tafamidis for the treatment of transthyretin amyloid cardiomyopathy (ATTR-ACT) trial.MethodsPatient-level data from the 30-mo ATTR-ACT trial were used to develop survival models based on parametric ACS and RS models. The latter was composed of an expected hazard and an independent excess hazard. Models were selected according to statistical goodness of fit and clinical plausibility, with extrapolation up to 72 mo validated against ATTR-ACT long-term extension (LTE) data.ResultsInformation criteria were too similar to discriminate between RS or ACS models. Several ACS models were affected by capping with general population mortality rates and considered implausible. Selected RS models matched the empirical hazard function, could not fall below general population hazards, and predicted well compared with the LTE data. The preferred RS model predicted the restricted mean survival (RMST) to 72 mo of 51.0 mo (95% confidence interval [CI]: 46.1, 55.3); this compared favorably to the LTE RMST of 50.9 mo (95% CI: 47.7, 53.9).DiscussionRS models can improve the accuracy for modeling populations with high background mortality rates (e.g., the ATTR-CM trial). RS modeling enforces a plausible long-term hazard profile, enables flexibility in medium-term hazard profiles, and increases the robustness of medical decision making.HighlightsTo inform survival extrapolations for health technology assessment, a relative survival model incorporating external data per the recommendations of the National Institute for Health and Care Excellence (NICE) Decision Support Unit was used in support of the NICE evaluation of tafamidis for treatment of transthyretin amyloid cardiomyopathy (ATTR-CM).Relative survival modeling allowed selection of a broader range of hazard profiles compared with all-cause survival modeling by ensuring plausible long-term predictions.Predictions from plausible relative survival models of overall survival in patients with ATTR-CM, extrapolated from the ATTR-ACT trial, validated very well to outcomes after a doubling of follow-up and demonstrated improved precision and accuracy versus parametric all-cause survival models.</p>","PeriodicalId":49839,"journal":{"name":"Medical Decision Making","volume":" ","pages":"726-739"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304488/pdf/","citationCount":"0","resultStr":"{\"title\":\"Relative Survival Modeling for Appraising the Cost-Effectiveness of Life-Extending Treatments: An Application to Tafamidis for the Treatment of Transthyretin Amyloidosis with Cardiomyopathy.\",\"authors\":\"Robert Young, Jack Said, Sam Large\",\"doi\":\"10.1177/0272989X251342459\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BackgroundEconomic evaluations for life-extending treatments frequently require clinical trial data to be extrapolated beyond the trial duration to estimate changes in life expectancy. Conventional survival models often display hazard profiles that do not rise as expected in an aging population and require the incorporation of external data to ensure plausibility. Relative survival (RS) models can enable the incorporation of external data at model fitting. A comparison was performed between RS and \\\"standard\\\" all-cause survival (ACS) in modeling outcomes from the tafamidis for the treatment of transthyretin amyloid cardiomyopathy (ATTR-ACT) trial.MethodsPatient-level data from the 30-mo ATTR-ACT trial were used to develop survival models based on parametric ACS and RS models. The latter was composed of an expected hazard and an independent excess hazard. Models were selected according to statistical goodness of fit and clinical plausibility, with extrapolation up to 72 mo validated against ATTR-ACT long-term extension (LTE) data.ResultsInformation criteria were too similar to discriminate between RS or ACS models. Several ACS models were affected by capping with general population mortality rates and considered implausible. Selected RS models matched the empirical hazard function, could not fall below general population hazards, and predicted well compared with the LTE data. The preferred RS model predicted the restricted mean survival (RMST) to 72 mo of 51.0 mo (95% confidence interval [CI]: 46.1, 55.3); this compared favorably to the LTE RMST of 50.9 mo (95% CI: 47.7, 53.9).DiscussionRS models can improve the accuracy for modeling populations with high background mortality rates (e.g., the ATTR-CM trial). RS modeling enforces a plausible long-term hazard profile, enables flexibility in medium-term hazard profiles, and increases the robustness of medical decision making.HighlightsTo inform survival extrapolations for health technology assessment, a relative survival model incorporating external data per the recommendations of the National Institute for Health and Care Excellence (NICE) Decision Support Unit was used in support of the NICE evaluation of tafamidis for treatment of transthyretin amyloid cardiomyopathy (ATTR-CM).Relative survival modeling allowed selection of a broader range of hazard profiles compared with all-cause survival modeling by ensuring plausible long-term predictions.Predictions from plausible relative survival models of overall survival in patients with ATTR-CM, extrapolated from the ATTR-ACT trial, validated very well to outcomes after a doubling of follow-up and demonstrated improved precision and accuracy versus parametric all-cause survival models.</p>\",\"PeriodicalId\":49839,\"journal\":{\"name\":\"Medical Decision Making\",\"volume\":\" \",\"pages\":\"726-739\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304488/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Decision Making\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/0272989X251342459\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Decision Making","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/0272989X251342459","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Relative Survival Modeling for Appraising the Cost-Effectiveness of Life-Extending Treatments: An Application to Tafamidis for the Treatment of Transthyretin Amyloidosis with Cardiomyopathy.
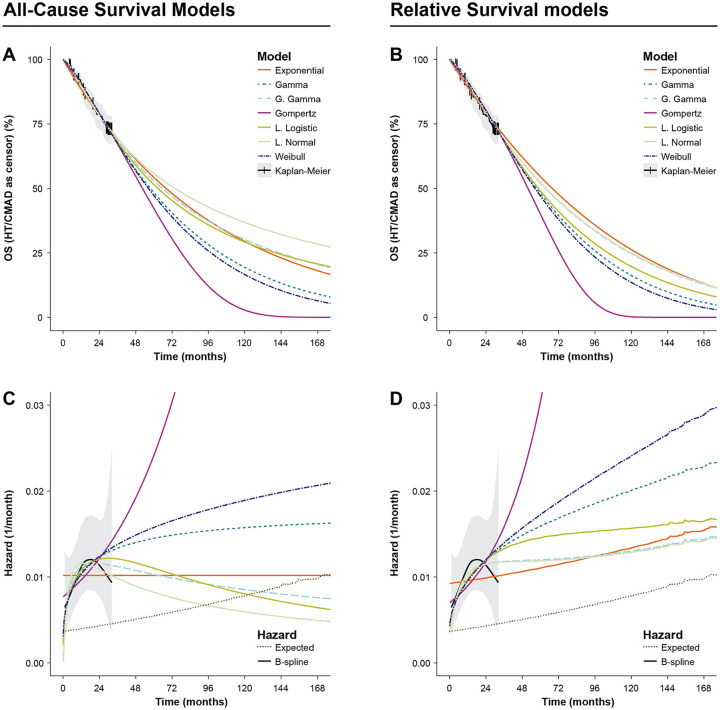
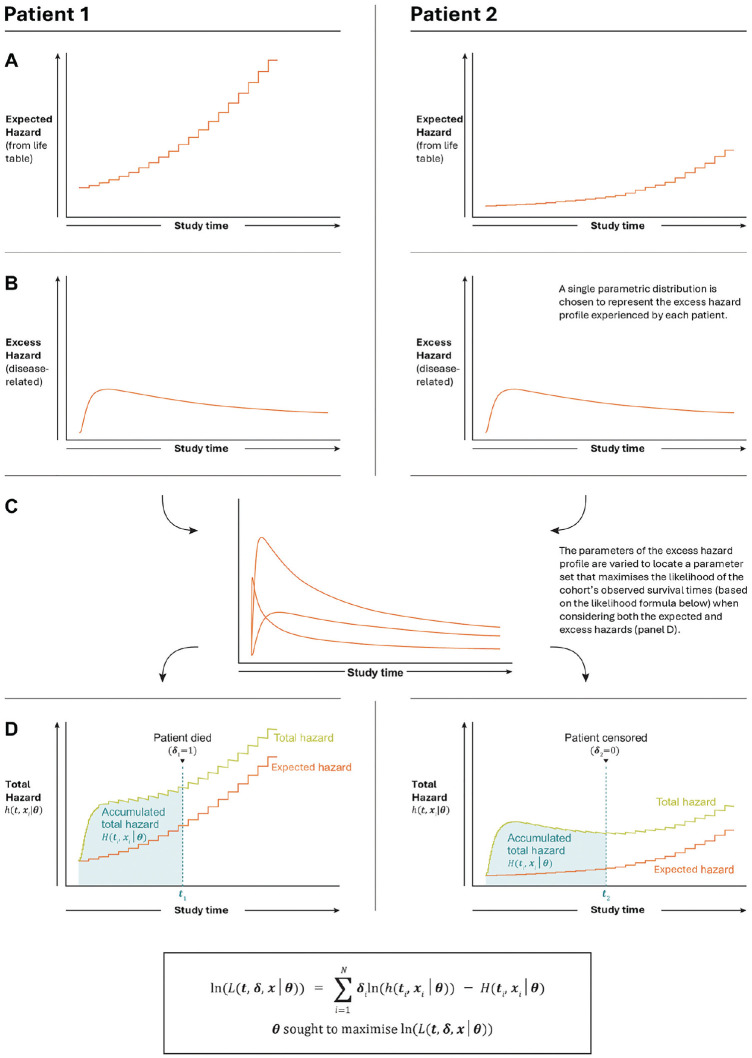
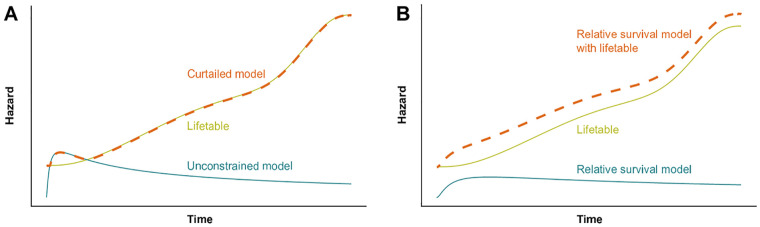
BackgroundEconomic evaluations for life-extending treatments frequently require clinical trial data to be extrapolated beyond the trial duration to estimate changes in life expectancy. Conventional survival models often display hazard profiles that do not rise as expected in an aging population and require the incorporation of external data to ensure plausibility. Relative survival (RS) models can enable the incorporation of external data at model fitting. A comparison was performed between RS and "standard" all-cause survival (ACS) in modeling outcomes from the tafamidis for the treatment of transthyretin amyloid cardiomyopathy (ATTR-ACT) trial.MethodsPatient-level data from the 30-mo ATTR-ACT trial were used to develop survival models based on parametric ACS and RS models. The latter was composed of an expected hazard and an independent excess hazard. Models were selected according to statistical goodness of fit and clinical plausibility, with extrapolation up to 72 mo validated against ATTR-ACT long-term extension (LTE) data.ResultsInformation criteria were too similar to discriminate between RS or ACS models. Several ACS models were affected by capping with general population mortality rates and considered implausible. Selected RS models matched the empirical hazard function, could not fall below general population hazards, and predicted well compared with the LTE data. The preferred RS model predicted the restricted mean survival (RMST) to 72 mo of 51.0 mo (95% confidence interval [CI]: 46.1, 55.3); this compared favorably to the LTE RMST of 50.9 mo (95% CI: 47.7, 53.9).DiscussionRS models can improve the accuracy for modeling populations with high background mortality rates (e.g., the ATTR-CM trial). RS modeling enforces a plausible long-term hazard profile, enables flexibility in medium-term hazard profiles, and increases the robustness of medical decision making.HighlightsTo inform survival extrapolations for health technology assessment, a relative survival model incorporating external data per the recommendations of the National Institute for Health and Care Excellence (NICE) Decision Support Unit was used in support of the NICE evaluation of tafamidis for treatment of transthyretin amyloid cardiomyopathy (ATTR-CM).Relative survival modeling allowed selection of a broader range of hazard profiles compared with all-cause survival modeling by ensuring plausible long-term predictions.Predictions from plausible relative survival models of overall survival in patients with ATTR-CM, extrapolated from the ATTR-ACT trial, validated very well to outcomes after a doubling of follow-up and demonstrated improved precision and accuracy versus parametric all-cause survival models.
期刊介绍:
Medical Decision Making offers rigorous and systematic approaches to decision making that are designed to improve the health and clinical care of individuals and to assist with health care policy development. Using the fundamentals of decision analysis and theory, economic evaluation, and evidence based quality assessment, Medical Decision Making presents both theoretical and practical statistical and modeling techniques and methods from a variety of disciplines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


