Chenhao Dou, Qingsong Yu, Wei Zhang, Lei Ma, Xianzhong Meng
{"title":"双门静脉内窥镜技术与传统单侧椎板切除术治疗老年人多层次退行性腰椎管狭窄症的比较。","authors":"Chenhao Dou, Qingsong Yu, Wei Zhang, Lei Ma, Xianzhong Meng","doi":"10.1111/os.70084","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The object of this retrospective study was to compare the clinical, radiological, and spinal stability outcomes of biportal endoscopic Unilateral Laminectomy for Bilateral Decompression (BE-ULBD) and traditional Unilateral Laminectomy for Bilateral Decompression (ULBD) for multi-segmental lumbar spinal stenosis in elderly patients with osteoporosis.</p><p><strong>Methods: </strong>We retrospectively identified 41 and 47 patients who underwent BE-ULBD and ULBD, respectively, who were diagnosed with multi-level lumbar stenosis and underwent double-segmental surgery in elderly patients. The clinical outcomes were evaluated using visual analogue scale (VAS) score for both back and leg pain, Oswestry Disability Index (ODI) score, and Zurich Claudication Questionnaire score during the two-year follow-up. The radiological changes of cross-sectional dural area (DCSA), facet joint preservation rate (PFJR) and cross-sectional fat infiltration ratio (FI) on the surgical side were evaluated by MRI before and after operation. At 2 years after operation, progressive spondylolisthesis and instability were evaluated in the X-ray of the lumbar spine.</p><p><strong>Results: </strong>After 24 months of follow-up, the VAS scores for both back and leg pain, ODI, and Zurich Claudication Questionnaire in both groups were recovered compared to pre-operation. The postoperative VAS score for lower back pain in the BE-ULBD group was lower than in the ULBD group (1.00 ± 0.95 vs. 1.91 ± 1.07, p < 0.001), and the postoperative VAS score for lower limbs was similar (0.49 ± 0.51 vs. 0.46 ± 0.72, p < 0.001). The postoperative ODI score was lower than that of the ULBD group (9.05 ± 5.01 vs. 12.09 ± 6.18, p < 0.001), and the postoperative ZCQ score of the BE-ULBD group was lower than that of the ULBD group (10.59 ± 2.18 vs. 8.85 ± 1.59, p < 0.001; 7.00 ± 1.12 vs. 7.87 ± 1.63, p = 0.012; 8.95 ± 2.11 vs. 10.74 ± 2.47, p < 0.001). In terms of radiological evaluation, the DCSA of patients in both groups was effectively improved after surgery. Compared with the ULBD group, the BE-ULBD group had a tiny improvement in DCSA (195.04 ± 34.54 vs. 180.93 ± 31.07, p = 0.048) and a better FI (43.48 ± 10.24 vs. 53.93 ± 7.62, p < 0.001). The PFJR was higher (85.90 ± 4.03 vs. 81.26 ± 4.56, p < 0.001) in the BE-ULBD group. Two years after surgery, fewer patients in the BE-ULBD group had spondylolisthesis than in the ULBD group (1/41 vs. 7/46, p = 0.043). The results of complications were similar between the two groups.</p><p><strong>Conclusion: </strong>BE-ULBD is a safe and effective technique for multilevel decompression surgery in elderly patients, which can better protect spinal stability and has better long-term follow-up than traditional surgery.</p>","PeriodicalId":19566,"journal":{"name":"Orthopaedic Surgery","volume":" ","pages":"2302-2312"},"PeriodicalIF":2.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318692/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Biportal Endoscopic Technique and Conventional Unilateral Laminectomy for Bilateral Decompression (ULBD) for Multi-Level Degenerative Lumbar Spinal Stenosis in Elderly People.\",\"authors\":\"Chenhao Dou, Qingsong Yu, Wei Zhang, Lei Ma, Xianzhong Meng\",\"doi\":\"10.1111/os.70084\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The object of this retrospective study was to compare the clinical, radiological, and spinal stability outcomes of biportal endoscopic Unilateral Laminectomy for Bilateral Decompression (BE-ULBD) and traditional Unilateral Laminectomy for Bilateral Decompression (ULBD) for multi-segmental lumbar spinal stenosis in elderly patients with osteoporosis.</p><p><strong>Methods: </strong>We retrospectively identified 41 and 47 patients who underwent BE-ULBD and ULBD, respectively, who were diagnosed with multi-level lumbar stenosis and underwent double-segmental surgery in elderly patients. The clinical outcomes were evaluated using visual analogue scale (VAS) score for both back and leg pain, Oswestry Disability Index (ODI) score, and Zurich Claudication Questionnaire score during the two-year follow-up. The radiological changes of cross-sectional dural area (DCSA), facet joint preservation rate (PFJR) and cross-sectional fat infiltration ratio (FI) on the surgical side were evaluated by MRI before and after operation. At 2 years after operation, progressive spondylolisthesis and instability were evaluated in the X-ray of the lumbar spine.</p><p><strong>Results: </strong>After 24 months of follow-up, the VAS scores for both back and leg pain, ODI, and Zurich Claudication Questionnaire in both groups were recovered compared to pre-operation. The postoperative VAS score for lower back pain in the BE-ULBD group was lower than in the ULBD group (1.00 ± 0.95 vs. 1.91 ± 1.07, p < 0.001), and the postoperative VAS score for lower limbs was similar (0.49 ± 0.51 vs. 0.46 ± 0.72, p < 0.001). The postoperative ODI score was lower than that of the ULBD group (9.05 ± 5.01 vs. 12.09 ± 6.18, p < 0.001), and the postoperative ZCQ score of the BE-ULBD group was lower than that of the ULBD group (10.59 ± 2.18 vs. 8.85 ± 1.59, p < 0.001; 7.00 ± 1.12 vs. 7.87 ± 1.63, p = 0.012; 8.95 ± 2.11 vs. 10.74 ± 2.47, p < 0.001). In terms of radiological evaluation, the DCSA of patients in both groups was effectively improved after surgery. Compared with the ULBD group, the BE-ULBD group had a tiny improvement in DCSA (195.04 ± 34.54 vs. 180.93 ± 31.07, p = 0.048) and a better FI (43.48 ± 10.24 vs. 53.93 ± 7.62, p < 0.001). The PFJR was higher (85.90 ± 4.03 vs. 81.26 ± 4.56, p < 0.001) in the BE-ULBD group. Two years after surgery, fewer patients in the BE-ULBD group had spondylolisthesis than in the ULBD group (1/41 vs. 7/46, p = 0.043). The results of complications were similar between the two groups.</p><p><strong>Conclusion: </strong>BE-ULBD is a safe and effective technique for multilevel decompression surgery in elderly patients, which can better protect spinal stability and has better long-term follow-up than traditional surgery.</p>\",\"PeriodicalId\":19566,\"journal\":{\"name\":\"Orthopaedic Surgery\",\"volume\":\" \",\"pages\":\"2302-2312\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318692/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Orthopaedic Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/os.70084\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/os.70084","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Comparison of Biportal Endoscopic Technique and Conventional Unilateral Laminectomy for Bilateral Decompression (ULBD) for Multi-Level Degenerative Lumbar Spinal Stenosis in Elderly People.
Objective: The object of this retrospective study was to compare the clinical, radiological, and spinal stability outcomes of biportal endoscopic Unilateral Laminectomy for Bilateral Decompression (BE-ULBD) and traditional Unilateral Laminectomy for Bilateral Decompression (ULBD) for multi-segmental lumbar spinal stenosis in elderly patients with osteoporosis.
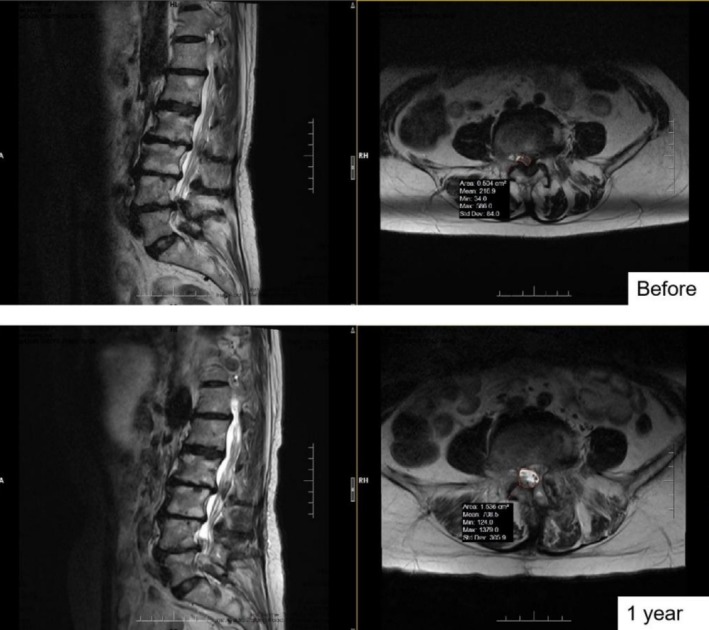
Methods: We retrospectively identified 41 and 47 patients who underwent BE-ULBD and ULBD, respectively, who were diagnosed with multi-level lumbar stenosis and underwent double-segmental surgery in elderly patients. The clinical outcomes were evaluated using visual analogue scale (VAS) score for both back and leg pain, Oswestry Disability Index (ODI) score, and Zurich Claudication Questionnaire score during the two-year follow-up. The radiological changes of cross-sectional dural area (DCSA), facet joint preservation rate (PFJR) and cross-sectional fat infiltration ratio (FI) on the surgical side were evaluated by MRI before and after operation. At 2 years after operation, progressive spondylolisthesis and instability were evaluated in the X-ray of the lumbar spine.
Results: After 24 months of follow-up, the VAS scores for both back and leg pain, ODI, and Zurich Claudication Questionnaire in both groups were recovered compared to pre-operation. The postoperative VAS score for lower back pain in the BE-ULBD group was lower than in the ULBD group (1.00 ± 0.95 vs. 1.91 ± 1.07, p < 0.001), and the postoperative VAS score for lower limbs was similar (0.49 ± 0.51 vs. 0.46 ± 0.72, p < 0.001). The postoperative ODI score was lower than that of the ULBD group (9.05 ± 5.01 vs. 12.09 ± 6.18, p < 0.001), and the postoperative ZCQ score of the BE-ULBD group was lower than that of the ULBD group (10.59 ± 2.18 vs. 8.85 ± 1.59, p < 0.001; 7.00 ± 1.12 vs. 7.87 ± 1.63, p = 0.012; 8.95 ± 2.11 vs. 10.74 ± 2.47, p < 0.001). In terms of radiological evaluation, the DCSA of patients in both groups was effectively improved after surgery. Compared with the ULBD group, the BE-ULBD group had a tiny improvement in DCSA (195.04 ± 34.54 vs. 180.93 ± 31.07, p = 0.048) and a better FI (43.48 ± 10.24 vs. 53.93 ± 7.62, p < 0.001). The PFJR was higher (85.90 ± 4.03 vs. 81.26 ± 4.56, p < 0.001) in the BE-ULBD group. Two years after surgery, fewer patients in the BE-ULBD group had spondylolisthesis than in the ULBD group (1/41 vs. 7/46, p = 0.043). The results of complications were similar between the two groups.
Conclusion: BE-ULBD is a safe and effective technique for multilevel decompression surgery in elderly patients, which can better protect spinal stability and has better long-term follow-up than traditional surgery.
期刊介绍:
Orthopaedic Surgery (OS) is the official journal of the Chinese Orthopaedic Association, focusing on all aspects of orthopaedic technique and surgery.
The journal publishes peer-reviewed articles in the following categories: Original Articles, Clinical Articles, Review Articles, Guidelines, Editorials, Commentaries, Surgical Techniques, Case Reports and Meeting Reports.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


