Renée J G Arnold, Winona Tse, Kimberly Martin, Renee Kuan
{"title":"帕金森病患者医疗保险受益人的医疗保健利用、治疗模式和经济负担的现实世界分析:左旋多巴制剂和疾病严重程度的影响","authors":"Renée J G Arnold, Winona Tse, Kimberly Martin, Renee Kuan","doi":"10.1007/s41669-025-00588-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to evaluate healthcare utilization, costs, and treatment patterns of Medicare beneficiaries with Parkinson's disease (PD) treated with different carbidopa-levodopa regimens.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted using 100% fee-for-service Medicare research identifiable claims data from 2017 to 2019. The study population included 201,241 Medicare beneficiaries aged 65-90 years with PD who received at least one prescription for a carbidopa-levodopa-containing regimen. Treatment patterns, healthcare resource utilization, and costs were analyzed, stratified by medication regimen containing levodopa and levodopa equivalent daily dose (LEDD), the latter as a proxy for disease severity.</p><p><strong>Results: </strong>Immediate release (IR) carbidopa-levodopa was the most common initial prescription (83%). Extended release (ER) formulations had the highest mean daily dose (1140 mg, although the equivalent dose in a non-ER formulation is approximately 570 mg, in line with the other three primary regimens). Treatment persistence and cost generally increased with higher LEDD. Concomitant medication use, particularly dopamine agonists, also increased with higher LEDD. Total 3-year per patient healthcare costs were lower for patients prescribed controlled release (CR) carbidopa-levodopa (US $98,650); compared with US $116,394 for patients prescribed IR carbidopa-levodopa; US $123,650 for those prescribed CR + IR carbidopa-levodopa; and US $125,802 for ER carbidopa-levodopa. Costs tended to increase with higher LEDD, primarily driven by outpatient care and medications.</p><p><strong>Conclusions: </strong>This study provides comprehensive real-world evidence on carbidopa-levodopa use in Medicare beneficiaries with PD. Findings highlight the need for individualized treatment approaches, considering both symptom control and healthcare costs. Future research should focus on prospective studies to assess long-term outcomes and economic impact of different treatment strategies in PD, considering disease severity and quality of life.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"771-783"},"PeriodicalIF":2.1000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401846/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-World Analysis of Healthcare Utilization, Treatment Patterns, and Economic Burden in Medicare Beneficiaries with Parkinson's Disease: Implications by Levodopa Formulation and Disease Severity.\",\"authors\":\"Renée J G Arnold, Winona Tse, Kimberly Martin, Renee Kuan\",\"doi\":\"10.1007/s41669-025-00588-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study aimed to evaluate healthcare utilization, costs, and treatment patterns of Medicare beneficiaries with Parkinson's disease (PD) treated with different carbidopa-levodopa regimens.</p><p><strong>Methods: </strong>A retrospective cohort study was conducted using 100% fee-for-service Medicare research identifiable claims data from 2017 to 2019. The study population included 201,241 Medicare beneficiaries aged 65-90 years with PD who received at least one prescription for a carbidopa-levodopa-containing regimen. Treatment patterns, healthcare resource utilization, and costs were analyzed, stratified by medication regimen containing levodopa and levodopa equivalent daily dose (LEDD), the latter as a proxy for disease severity.</p><p><strong>Results: </strong>Immediate release (IR) carbidopa-levodopa was the most common initial prescription (83%). Extended release (ER) formulations had the highest mean daily dose (1140 mg, although the equivalent dose in a non-ER formulation is approximately 570 mg, in line with the other three primary regimens). Treatment persistence and cost generally increased with higher LEDD. Concomitant medication use, particularly dopamine agonists, also increased with higher LEDD. Total 3-year per patient healthcare costs were lower for patients prescribed controlled release (CR) carbidopa-levodopa (US $98,650); compared with US $116,394 for patients prescribed IR carbidopa-levodopa; US $123,650 for those prescribed CR + IR carbidopa-levodopa; and US $125,802 for ER carbidopa-levodopa. Costs tended to increase with higher LEDD, primarily driven by outpatient care and medications.</p><p><strong>Conclusions: </strong>This study provides comprehensive real-world evidence on carbidopa-levodopa use in Medicare beneficiaries with PD. Findings highlight the need for individualized treatment approaches, considering both symptom control and healthcare costs. Future research should focus on prospective studies to assess long-term outcomes and economic impact of different treatment strategies in PD, considering disease severity and quality of life.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"771-783\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401846/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-025-00588-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-025-00588-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Real-World Analysis of Healthcare Utilization, Treatment Patterns, and Economic Burden in Medicare Beneficiaries with Parkinson's Disease: Implications by Levodopa Formulation and Disease Severity.
Objective: This study aimed to evaluate healthcare utilization, costs, and treatment patterns of Medicare beneficiaries with Parkinson's disease (PD) treated with different carbidopa-levodopa regimens.
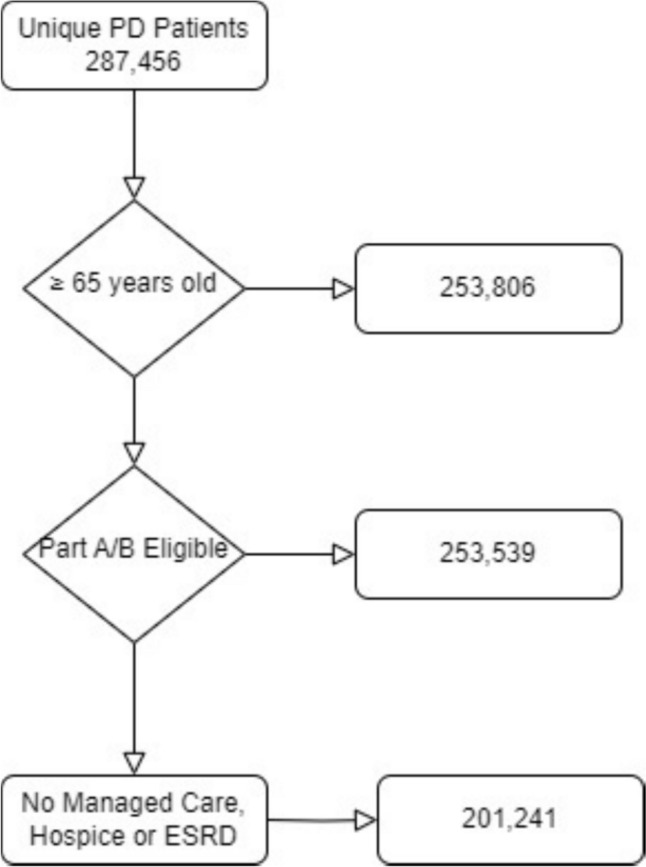
Methods: A retrospective cohort study was conducted using 100% fee-for-service Medicare research identifiable claims data from 2017 to 2019. The study population included 201,241 Medicare beneficiaries aged 65-90 years with PD who received at least one prescription for a carbidopa-levodopa-containing regimen. Treatment patterns, healthcare resource utilization, and costs were analyzed, stratified by medication regimen containing levodopa and levodopa equivalent daily dose (LEDD), the latter as a proxy for disease severity.
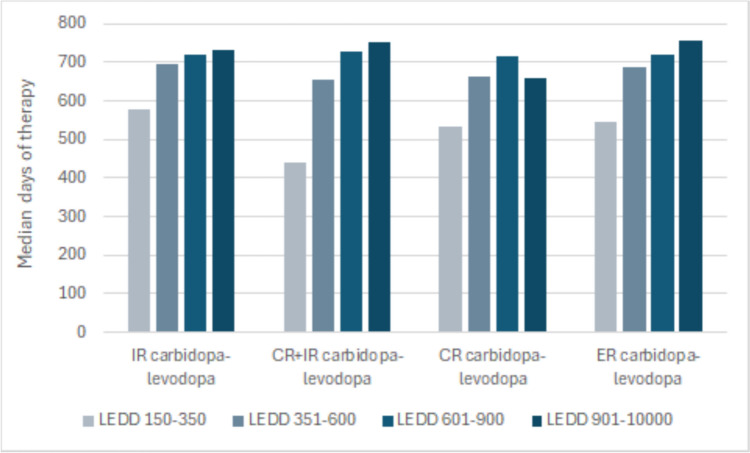
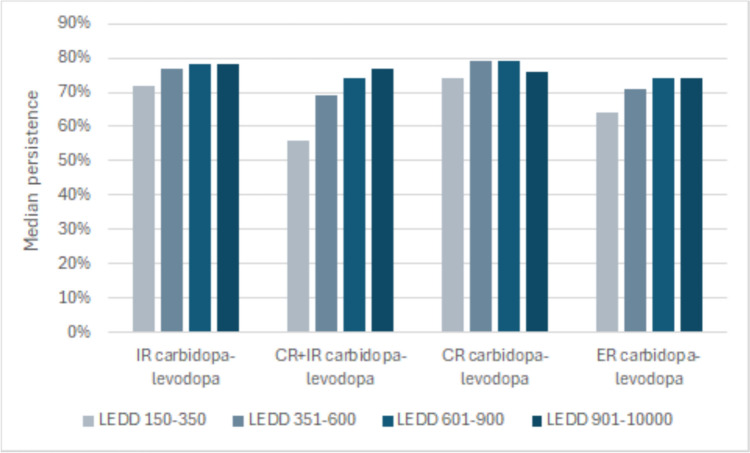
Results: Immediate release (IR) carbidopa-levodopa was the most common initial prescription (83%). Extended release (ER) formulations had the highest mean daily dose (1140 mg, although the equivalent dose in a non-ER formulation is approximately 570 mg, in line with the other three primary regimens). Treatment persistence and cost generally increased with higher LEDD. Concomitant medication use, particularly dopamine agonists, also increased with higher LEDD. Total 3-year per patient healthcare costs were lower for patients prescribed controlled release (CR) carbidopa-levodopa (US $98,650); compared with US $116,394 for patients prescribed IR carbidopa-levodopa; US $123,650 for those prescribed CR + IR carbidopa-levodopa; and US $125,802 for ER carbidopa-levodopa. Costs tended to increase with higher LEDD, primarily driven by outpatient care and medications.
Conclusions: This study provides comprehensive real-world evidence on carbidopa-levodopa use in Medicare beneficiaries with PD. Findings highlight the need for individualized treatment approaches, considering both symptom control and healthcare costs. Future research should focus on prospective studies to assess long-term outcomes and economic impact of different treatment strategies in PD, considering disease severity and quality of life.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


