Marc M Terpstra, Tim A C de Vries, Ellis Oortwijn, Rob A F de Lind van Wijngaarden, Joris R de Groot
{"title":"口服抗凝剂的类型对心脏手术后房颤患者卒中预防或出血有影响吗?系统回顾和荟萃分析。","authors":"Marc M Terpstra, Tim A C de Vries, Ellis Oortwijn, Rob A F de Lind van Wijngaarden, Joris R de Groot","doi":"10.1093/ehjopen/oeaf062","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Unlike in non-surgical settings, many centres continue to favour vitamin K antagonists (VKAs) for stroke prevention in atrial fibrillation (AF) following major cardiac surgery. Current guidelines indicate insufficient data on the use of direct oral anticoagulants (DOACs) early after cardiac surgery. This study aims to evaluate whether DOACs are non-inferior to VKAs in terms of efficacy and safety for stroke prevention in post-operative AF.</p><p><strong>Methods and results: </strong>MEDLINE, EMBASE, CENTRAL, and Clinicaltrials.gov were searched from inception till 2 July 2024, and relevant reviews were screened as grey literature. Studies comparing DOACs with VKAs for stroke prevention in patients with (post-operative) AF after major cardiac surgery were included. Studies on patients with mechanical valve replacement or moderate to severe mitral stenosis were excluded. Outcomes of interest included thromboembolic events, major bleeding and mortality up to 6 months after cardiac surgery. Eleven studies, including two randomized controlled trials, reporting on >18,000 patients were analyzed. There were no significant differences between DOACs and VKAs in thromboembolic events (OR: 0.96; CI: 0.62-1.50; I<sup>2</sup>: 0%), any stroke (OR: 1.44; CI: 0.61-3.41; I<sup>2</sup>: 0%), major bleeding (OR: 0.97; CI: 0.60-1.56; I<sup>2</sup>: 48%), all-cause mortality (OR: 1.00; CI: 0.73-1.37; I<sup>2</sup>: 0%) or admission duration (MD: -0.33; CI: -1.16-0.49; I<sup>2</sup>: 0%) in the first 6 months after cardiac surgery.</p><p><strong>Conclusion: </strong>There is no high-quality evidence that DOACs and VKAs differ in efficacy or safety for stroke prevention in AF after cardiac surgery. While awaiting high-quality randomized data, our meta-analysis found no evidence to support routinely avoiding DOACs or favouring VKAs in this setting.</p><p><strong>Registration: </strong>Review registration number: CRD42023412592.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf062"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12166522/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does the type of oral anticoagulant matter for stroke prevention or bleeding in patients with atrial fibrillation after cardiac surgery? A systematic review and meta-analysis.\",\"authors\":\"Marc M Terpstra, Tim A C de Vries, Ellis Oortwijn, Rob A F de Lind van Wijngaarden, Joris R de Groot\",\"doi\":\"10.1093/ehjopen/oeaf062\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Unlike in non-surgical settings, many centres continue to favour vitamin K antagonists (VKAs) for stroke prevention in atrial fibrillation (AF) following major cardiac surgery. Current guidelines indicate insufficient data on the use of direct oral anticoagulants (DOACs) early after cardiac surgery. This study aims to evaluate whether DOACs are non-inferior to VKAs in terms of efficacy and safety for stroke prevention in post-operative AF.</p><p><strong>Methods and results: </strong>MEDLINE, EMBASE, CENTRAL, and Clinicaltrials.gov were searched from inception till 2 July 2024, and relevant reviews were screened as grey literature. Studies comparing DOACs with VKAs for stroke prevention in patients with (post-operative) AF after major cardiac surgery were included. Studies on patients with mechanical valve replacement or moderate to severe mitral stenosis were excluded. Outcomes of interest included thromboembolic events, major bleeding and mortality up to 6 months after cardiac surgery. Eleven studies, including two randomized controlled trials, reporting on >18,000 patients were analyzed. There were no significant differences between DOACs and VKAs in thromboembolic events (OR: 0.96; CI: 0.62-1.50; I<sup>2</sup>: 0%), any stroke (OR: 1.44; CI: 0.61-3.41; I<sup>2</sup>: 0%), major bleeding (OR: 0.97; CI: 0.60-1.56; I<sup>2</sup>: 48%), all-cause mortality (OR: 1.00; CI: 0.73-1.37; I<sup>2</sup>: 0%) or admission duration (MD: -0.33; CI: -1.16-0.49; I<sup>2</sup>: 0%) in the first 6 months after cardiac surgery.</p><p><strong>Conclusion: </strong>There is no high-quality evidence that DOACs and VKAs differ in efficacy or safety for stroke prevention in AF after cardiac surgery. While awaiting high-quality randomized data, our meta-analysis found no evidence to support routinely avoiding DOACs or favouring VKAs in this setting.</p><p><strong>Registration: </strong>Review registration number: CRD42023412592.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf062\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12166522/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf062\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Does the type of oral anticoagulant matter for stroke prevention or bleeding in patients with atrial fibrillation after cardiac surgery? A systematic review and meta-analysis.
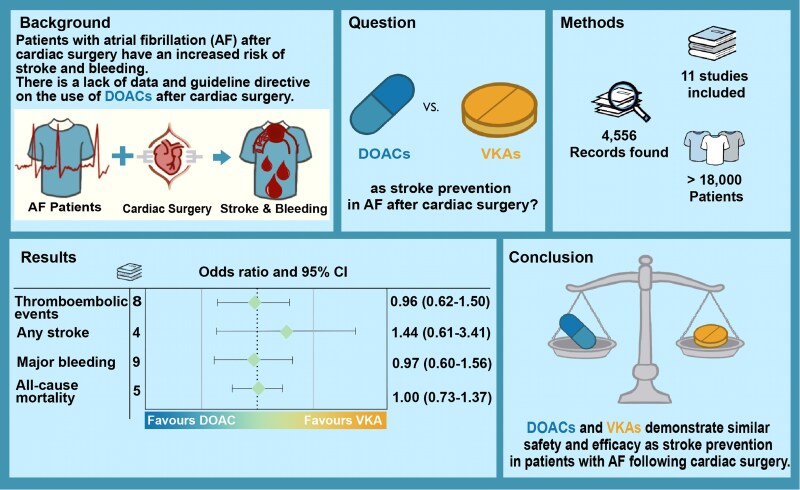
Aims: Unlike in non-surgical settings, many centres continue to favour vitamin K antagonists (VKAs) for stroke prevention in atrial fibrillation (AF) following major cardiac surgery. Current guidelines indicate insufficient data on the use of direct oral anticoagulants (DOACs) early after cardiac surgery. This study aims to evaluate whether DOACs are non-inferior to VKAs in terms of efficacy and safety for stroke prevention in post-operative AF.
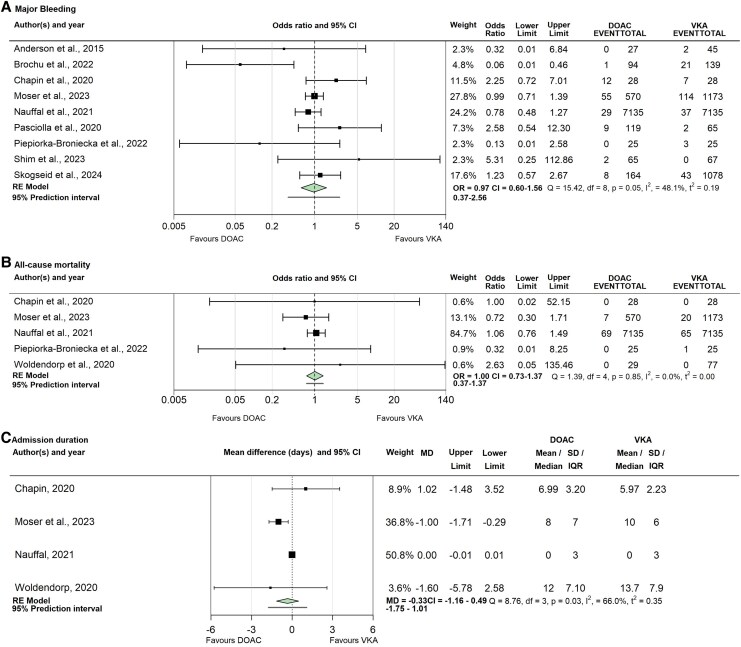
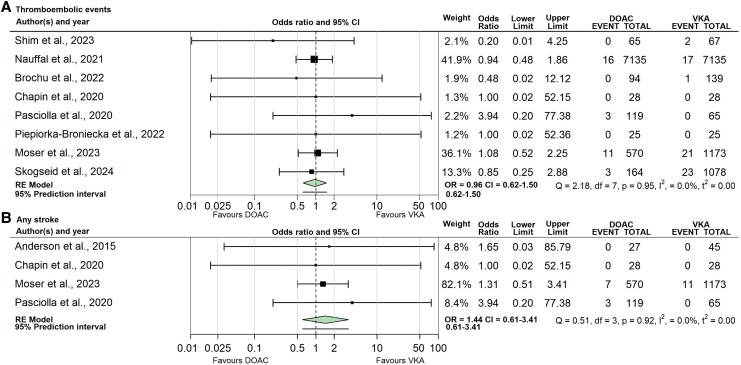
Methods and results: MEDLINE, EMBASE, CENTRAL, and Clinicaltrials.gov were searched from inception till 2 July 2024, and relevant reviews were screened as grey literature. Studies comparing DOACs with VKAs for stroke prevention in patients with (post-operative) AF after major cardiac surgery were included. Studies on patients with mechanical valve replacement or moderate to severe mitral stenosis were excluded. Outcomes of interest included thromboembolic events, major bleeding and mortality up to 6 months after cardiac surgery. Eleven studies, including two randomized controlled trials, reporting on >18,000 patients were analyzed. There were no significant differences between DOACs and VKAs in thromboembolic events (OR: 0.96; CI: 0.62-1.50; I2: 0%), any stroke (OR: 1.44; CI: 0.61-3.41; I2: 0%), major bleeding (OR: 0.97; CI: 0.60-1.56; I2: 48%), all-cause mortality (OR: 1.00; CI: 0.73-1.37; I2: 0%) or admission duration (MD: -0.33; CI: -1.16-0.49; I2: 0%) in the first 6 months after cardiac surgery.
Conclusion: There is no high-quality evidence that DOACs and VKAs differ in efficacy or safety for stroke prevention in AF after cardiac surgery. While awaiting high-quality randomized data, our meta-analysis found no evidence to support routinely avoiding DOACs or favouring VKAs in this setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


