Andrea Tumminia, Francesco Galeano, Vittorio Oteri, Federica Gambero, Stefania Panebianco, Roberto Baratta, Daniela Leonardi, Ilenia Marturano, Dario Giuffrida, Francesco Frasca, Damiano Gullo
{"title":"伴肾上腺偶发瘤的糖尿病患者严重迟发性阿比特龙诱导的低钾血症:一个诊断挑战。","authors":"Andrea Tumminia, Francesco Galeano, Vittorio Oteri, Federica Gambero, Stefania Panebianco, Roberto Baratta, Daniela Leonardi, Ilenia Marturano, Dario Giuffrida, Francesco Frasca, Damiano Gullo","doi":"10.1155/crie/8841993","DOIUrl":null,"url":null,"abstract":"<p><p>Prostate cancer is the most prevalent cancer among men in Western countries and is commonly managed by androgen deprivation therapy for locally advanced or metastatic stages. Even if initially effective, most patients eventually develop resistance to this treatment. Approved in 2011 for castration-resistant prostate cancer, abiraterone acetate inhibits the CYP17A1 enzyme, which is crucial in androgen and cortisol synthesis. This inhibition disrupts feedback on adrenocorticotropic hormone (ACTH), causing mineralocorticoid excess syndrome (MES), which is characterized by fluid retention, hypokalemia, and hypertension. MES can persist even with glucocorticoid supplementation, as observed in some cases. This study describes the case of a 68-year-old male with prostate cancer who developed severe, treatment-resistant hypokalemia after 6 years of abiraterone and prednisone therapy. The patient presented with poorly controlled diabetes and notable hypokalemia despite oral and parenteral potassium supplementation. Imaging revealed an adrenal adenoma; however, low renin and aldosterone levels suggested that abiraterone-induced MES, rather than primary aldosteronism, was responsible for his hypokalemia. The main therapy adjustment consisted of switching prednisone to dexamethasone to enhance ACTH suppression, effectively resolving the patient's hypokalemia. This case underscores the need for MES monitoring in patients on abiraterone, as MES can develop or worsen over time. Physicians should consider dexamethasone over prednisone in persistent MES cases, always monitoring also for the risk of developing Cushing syndrome. Given the rising prostate cancer incidence, clinicians must remain vigilant for MES-related complications with abiraterone, including delayed-onset severe hypokalemia.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2025 ","pages":"8841993"},"PeriodicalIF":0.9000,"publicationDate":"2025-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12163200/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe Late-Onset Abiraterone-Induced Hypokalemia in a Diabetic Patient With Concomitant Adrenal Gland Incidentaloma: A Diagnostic Challenge.\",\"authors\":\"Andrea Tumminia, Francesco Galeano, Vittorio Oteri, Federica Gambero, Stefania Panebianco, Roberto Baratta, Daniela Leonardi, Ilenia Marturano, Dario Giuffrida, Francesco Frasca, Damiano Gullo\",\"doi\":\"10.1155/crie/8841993\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Prostate cancer is the most prevalent cancer among men in Western countries and is commonly managed by androgen deprivation therapy for locally advanced or metastatic stages. Even if initially effective, most patients eventually develop resistance to this treatment. Approved in 2011 for castration-resistant prostate cancer, abiraterone acetate inhibits the CYP17A1 enzyme, which is crucial in androgen and cortisol synthesis. This inhibition disrupts feedback on adrenocorticotropic hormone (ACTH), causing mineralocorticoid excess syndrome (MES), which is characterized by fluid retention, hypokalemia, and hypertension. MES can persist even with glucocorticoid supplementation, as observed in some cases. This study describes the case of a 68-year-old male with prostate cancer who developed severe, treatment-resistant hypokalemia after 6 years of abiraterone and prednisone therapy. The patient presented with poorly controlled diabetes and notable hypokalemia despite oral and parenteral potassium supplementation. Imaging revealed an adrenal adenoma; however, low renin and aldosterone levels suggested that abiraterone-induced MES, rather than primary aldosteronism, was responsible for his hypokalemia. The main therapy adjustment consisted of switching prednisone to dexamethasone to enhance ACTH suppression, effectively resolving the patient's hypokalemia. This case underscores the need for MES monitoring in patients on abiraterone, as MES can develop or worsen over time. Physicians should consider dexamethasone over prednisone in persistent MES cases, always monitoring also for the risk of developing Cushing syndrome. Given the rising prostate cancer incidence, clinicians must remain vigilant for MES-related complications with abiraterone, including delayed-onset severe hypokalemia.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2025 \",\"pages\":\"8841993\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12163200/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crie/8841993\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crie/8841993","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Severe Late-Onset Abiraterone-Induced Hypokalemia in a Diabetic Patient With Concomitant Adrenal Gland Incidentaloma: A Diagnostic Challenge.
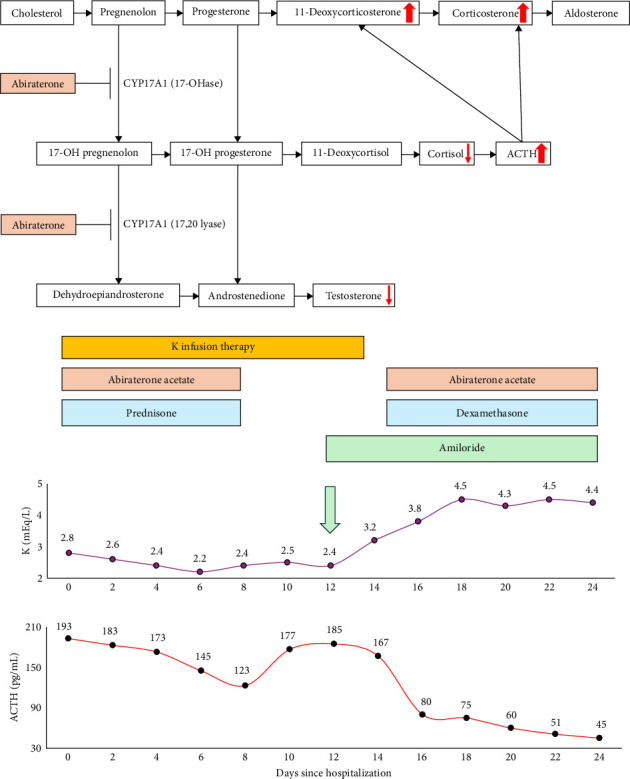
Prostate cancer is the most prevalent cancer among men in Western countries and is commonly managed by androgen deprivation therapy for locally advanced or metastatic stages. Even if initially effective, most patients eventually develop resistance to this treatment. Approved in 2011 for castration-resistant prostate cancer, abiraterone acetate inhibits the CYP17A1 enzyme, which is crucial in androgen and cortisol synthesis. This inhibition disrupts feedback on adrenocorticotropic hormone (ACTH), causing mineralocorticoid excess syndrome (MES), which is characterized by fluid retention, hypokalemia, and hypertension. MES can persist even with glucocorticoid supplementation, as observed in some cases. This study describes the case of a 68-year-old male with prostate cancer who developed severe, treatment-resistant hypokalemia after 6 years of abiraterone and prednisone therapy. The patient presented with poorly controlled diabetes and notable hypokalemia despite oral and parenteral potassium supplementation. Imaging revealed an adrenal adenoma; however, low renin and aldosterone levels suggested that abiraterone-induced MES, rather than primary aldosteronism, was responsible for his hypokalemia. The main therapy adjustment consisted of switching prednisone to dexamethasone to enhance ACTH suppression, effectively resolving the patient's hypokalemia. This case underscores the need for MES monitoring in patients on abiraterone, as MES can develop or worsen over time. Physicians should consider dexamethasone over prednisone in persistent MES cases, always monitoring also for the risk of developing Cushing syndrome. Given the rising prostate cancer incidence, clinicians must remain vigilant for MES-related complications with abiraterone, including delayed-onset severe hypokalemia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


