Federica Tramontana, Azmi Mohammed, Yaasir H Mamoojee, Richard Quinton
{"title":"睾酮诱导的红细胞增多症:解决代谢综合征和广泛处方sglt2抑制剂药物的挑战。","authors":"Federica Tramontana, Azmi Mohammed, Yaasir H Mamoojee, Richard Quinton","doi":"10.1530/EC-24-0695","DOIUrl":null,"url":null,"abstract":"<p><p>Testosterone is the cornerstone therapy for men with hypogonadism, and also treats any associated anaemia by promoting erythropoiesis. However, excessive doses cause erythrocytosis (raised red cell mass), especially if other risk factors are present. Erythrocytosis is associated with arterial and venous thrombosis in population studies. Testosterone is now increasingly prescribed to older men with functional hypogonadism and obesity, hypertension or type 2 diabetes, who are anyway at higher risk of both erythrocytosis and thrombosis. Although short-medium term testosterone treatment in these men was not associated with adverse cardiovascular outcomes, there were more cases of pulmonary embolism. Originally envisaged as purely oral hypoglycaemic drugs, sodium-glucose cotransporter 2 inhibitors (SGLT2i) are now increasingly prescribed in chronic kidney disease (CKD), ischaemic heart disease and left ventricular impairment, irrespective of glycaemia, and the likelihood of co-prescription with testosterone is thus increased considerably. Crucially, they also increase haematocrit by promoting haematopoiesis. This review focuses on the current best evidence for managing erythrocytosis, in the context of more prevalent obesity and prescriptions of testosterone and SGLT2i in this population. It highlights the need to balance the metabolic and therapeutic benefits against the potential risks. Management strategies include re-evaluating the original treatment indication, addressing modifiable risk factors, switching to transdermal testosterone and/or reducing the testosterone dose. Venesection is not recommended, except for clonal erythrocytosis, due to its potential pro-thrombotic effects. However, combination therapy with testosterone and SGLT2s in men with anaemia of advanced CKD could augment, or even partly supersede, expensive treatment with conventional erythrocytosis-stimulating agents.</p>","PeriodicalId":11634,"journal":{"name":"Endocrine Connections","volume":" ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12188712/pdf/","citationCount":"0","resultStr":"{\"title\":\"Testosterone-induced erythrocytosis: addressing the challenge of metabolic syndrome and widely prescribed SGLT2-inhibitor drugs.\",\"authors\":\"Federica Tramontana, Azmi Mohammed, Yaasir H Mamoojee, Richard Quinton\",\"doi\":\"10.1530/EC-24-0695\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Testosterone is the cornerstone therapy for men with hypogonadism, and also treats any associated anaemia by promoting erythropoiesis. However, excessive doses cause erythrocytosis (raised red cell mass), especially if other risk factors are present. Erythrocytosis is associated with arterial and venous thrombosis in population studies. Testosterone is now increasingly prescribed to older men with functional hypogonadism and obesity, hypertension or type 2 diabetes, who are anyway at higher risk of both erythrocytosis and thrombosis. Although short-medium term testosterone treatment in these men was not associated with adverse cardiovascular outcomes, there were more cases of pulmonary embolism. Originally envisaged as purely oral hypoglycaemic drugs, sodium-glucose cotransporter 2 inhibitors (SGLT2i) are now increasingly prescribed in chronic kidney disease (CKD), ischaemic heart disease and left ventricular impairment, irrespective of glycaemia, and the likelihood of co-prescription with testosterone is thus increased considerably. Crucially, they also increase haematocrit by promoting haematopoiesis. This review focuses on the current best evidence for managing erythrocytosis, in the context of more prevalent obesity and prescriptions of testosterone and SGLT2i in this population. It highlights the need to balance the metabolic and therapeutic benefits against the potential risks. Management strategies include re-evaluating the original treatment indication, addressing modifiable risk factors, switching to transdermal testosterone and/or reducing the testosterone dose. Venesection is not recommended, except for clonal erythrocytosis, due to its potential pro-thrombotic effects. However, combination therapy with testosterone and SGLT2s in men with anaemia of advanced CKD could augment, or even partly supersede, expensive treatment with conventional erythrocytosis-stimulating agents.</p>\",\"PeriodicalId\":11634,\"journal\":{\"name\":\"Endocrine Connections\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12188712/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine Connections\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1530/EC-24-0695\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"Print\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine Connections","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/EC-24-0695","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"Print","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Testosterone-induced erythrocytosis: addressing the challenge of metabolic syndrome and widely prescribed SGLT2-inhibitor drugs.
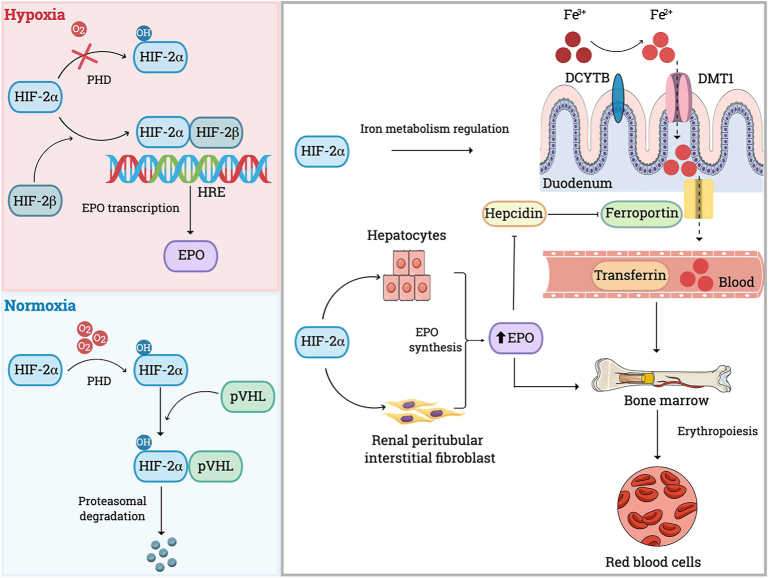
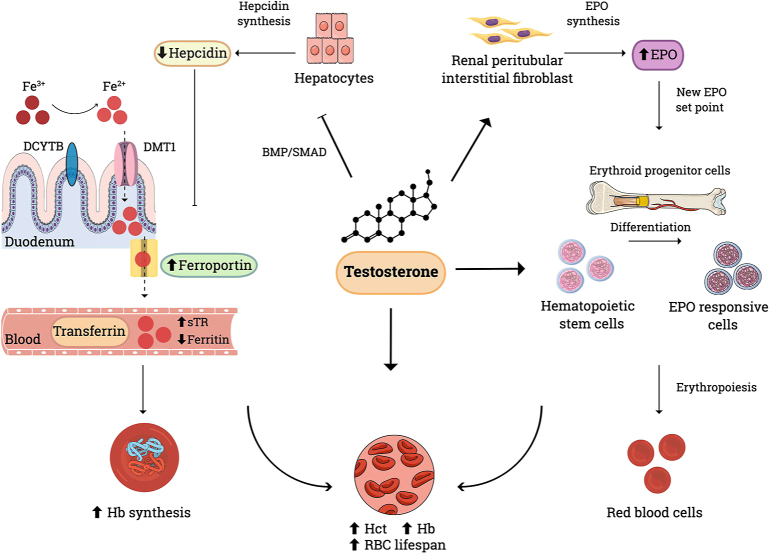
Testosterone is the cornerstone therapy for men with hypogonadism, and also treats any associated anaemia by promoting erythropoiesis. However, excessive doses cause erythrocytosis (raised red cell mass), especially if other risk factors are present. Erythrocytosis is associated with arterial and venous thrombosis in population studies. Testosterone is now increasingly prescribed to older men with functional hypogonadism and obesity, hypertension or type 2 diabetes, who are anyway at higher risk of both erythrocytosis and thrombosis. Although short-medium term testosterone treatment in these men was not associated with adverse cardiovascular outcomes, there were more cases of pulmonary embolism. Originally envisaged as purely oral hypoglycaemic drugs, sodium-glucose cotransporter 2 inhibitors (SGLT2i) are now increasingly prescribed in chronic kidney disease (CKD), ischaemic heart disease and left ventricular impairment, irrespective of glycaemia, and the likelihood of co-prescription with testosterone is thus increased considerably. Crucially, they also increase haematocrit by promoting haematopoiesis. This review focuses on the current best evidence for managing erythrocytosis, in the context of more prevalent obesity and prescriptions of testosterone and SGLT2i in this population. It highlights the need to balance the metabolic and therapeutic benefits against the potential risks. Management strategies include re-evaluating the original treatment indication, addressing modifiable risk factors, switching to transdermal testosterone and/or reducing the testosterone dose. Venesection is not recommended, except for clonal erythrocytosis, due to its potential pro-thrombotic effects. However, combination therapy with testosterone and SGLT2s in men with anaemia of advanced CKD could augment, or even partly supersede, expensive treatment with conventional erythrocytosis-stimulating agents.
期刊介绍:
Endocrine Connections publishes original quality research and reviews in all areas of endocrinology, including papers that deal with non-classical tissues as source or targets of hormones and endocrine papers that have relevance to endocrine-related and intersecting disciplines and the wider biomedical community.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


