Gareth J Williams, Daniel J Taylor, Abdulaziz Al Baraikan, Hazel Haley, Mina Ghobrial, Matthew Knight, Kenneth Anigboro, Vignesh Rammohan, Rebecca Gosling, Tom Newman, Mark Mills, Rod Hose, David A Wood, John A Cairns, Chinthanie Ramasundarahettige, Rutaba Khatun, Helen Nguyen, Shamir R Mehta, Robert F Storey, Julian P Gunn, Paul D Morris
{"title":"STEMI和多血管疾病患者非罪魁祸首疾病的虚拟生理分析:COMPLETE试验的一个亚研究","authors":"Gareth J Williams, Daniel J Taylor, Abdulaziz Al Baraikan, Hazel Haley, Mina Ghobrial, Matthew Knight, Kenneth Anigboro, Vignesh Rammohan, Rebecca Gosling, Tom Newman, Mark Mills, Rod Hose, David A Wood, John A Cairns, Chinthanie Ramasundarahettige, Rutaba Khatun, Helen Nguyen, Shamir R Mehta, Robert F Storey, Julian P Gunn, Paul D Morris","doi":"10.1093/ehjopen/oeaf057","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>In the complete revascularization with multivessel PCI for myocardial infarction (COMPLETE) trial, staged complete revascularization in patients with ST-segment-elevation myocardial infarction (MI) reduced major adverse cardiovascular events compared with culprit-only revascularization. Inclusion was based on angiographic criteria.</p><p><strong>Objectives: </strong>We modelled non-culprit virtual fractional flow reserve (vFFR) and investigated interactions between physiological lesion severity and the benefits of complete revascularization in COMPLETE.</p><p><strong>Methods and results: </strong>All suitable angiograms from COMPLETE underwent software-based 3-dimensional (3D) arterial reconstruction and analysis of 3D-quantitative coronary angiography (QCA) and vFFR using computational fluid dynamics software. Physiological lesion significance was defined as vFFR ≤0.80 and was compared with operators' visual angiographic analysis, 2D-QCA and 3D-QCA. vFFR was computed in 635 patients (710 lesions). 302 patients (48%) had ≥1 physiologically significant lesion and 333 (52%) had none. 321 (45%) lesions were physiologically significant and 389 (55%) were not. There was no statistically significant interaction between physiological lesion significance and any of the trial co-primary or key secondary clinical outcomes, or an exploratory outcome of ischaemia-driven revascularization without preceding MI (all interaction <i>P</i> > 0.30). 3D-QCA predicted vFFR significance more accurately than visual and 2D-QCA (concordance 73% vs. 49% vs. 59%, respectively).</p><p><strong>Conclusion: </strong>In this virtual physiological substudy of the COMPLETE trial, 52% of patients lacked any physiologically significant lesions and the benefits of complete revascularization appeared to be independent of physiological lesion significance. 3D-QCA was a better predictor of physiological significance than either 2D-QCA or operator visual analysis. Further research is warranted to compare angiography-guided and physiology-guided complete revascularization strategies.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf057"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152305/pdf/","citationCount":"0","resultStr":"{\"title\":\"Virtual physiological analysis of non-culprit disease in patients with STEMI and multivessel disease: a substudy of the COMPLETE trial.\",\"authors\":\"Gareth J Williams, Daniel J Taylor, Abdulaziz Al Baraikan, Hazel Haley, Mina Ghobrial, Matthew Knight, Kenneth Anigboro, Vignesh Rammohan, Rebecca Gosling, Tom Newman, Mark Mills, Rod Hose, David A Wood, John A Cairns, Chinthanie Ramasundarahettige, Rutaba Khatun, Helen Nguyen, Shamir R Mehta, Robert F Storey, Julian P Gunn, Paul D Morris\",\"doi\":\"10.1093/ehjopen/oeaf057\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>In the complete revascularization with multivessel PCI for myocardial infarction (COMPLETE) trial, staged complete revascularization in patients with ST-segment-elevation myocardial infarction (MI) reduced major adverse cardiovascular events compared with culprit-only revascularization. Inclusion was based on angiographic criteria.</p><p><strong>Objectives: </strong>We modelled non-culprit virtual fractional flow reserve (vFFR) and investigated interactions between physiological lesion severity and the benefits of complete revascularization in COMPLETE.</p><p><strong>Methods and results: </strong>All suitable angiograms from COMPLETE underwent software-based 3-dimensional (3D) arterial reconstruction and analysis of 3D-quantitative coronary angiography (QCA) and vFFR using computational fluid dynamics software. Physiological lesion significance was defined as vFFR ≤0.80 and was compared with operators' visual angiographic analysis, 2D-QCA and 3D-QCA. vFFR was computed in 635 patients (710 lesions). 302 patients (48%) had ≥1 physiologically significant lesion and 333 (52%) had none. 321 (45%) lesions were physiologically significant and 389 (55%) were not. There was no statistically significant interaction between physiological lesion significance and any of the trial co-primary or key secondary clinical outcomes, or an exploratory outcome of ischaemia-driven revascularization without preceding MI (all interaction <i>P</i> > 0.30). 3D-QCA predicted vFFR significance more accurately than visual and 2D-QCA (concordance 73% vs. 49% vs. 59%, respectively).</p><p><strong>Conclusion: </strong>In this virtual physiological substudy of the COMPLETE trial, 52% of patients lacked any physiologically significant lesions and the benefits of complete revascularization appeared to be independent of physiological lesion significance. 3D-QCA was a better predictor of physiological significance than either 2D-QCA or operator visual analysis. Further research is warranted to compare angiography-guided and physiology-guided complete revascularization strategies.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 3\",\"pages\":\"oeaf057\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152305/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf057\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf057","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Virtual physiological analysis of non-culprit disease in patients with STEMI and multivessel disease: a substudy of the COMPLETE trial.
Aims: In the complete revascularization with multivessel PCI for myocardial infarction (COMPLETE) trial, staged complete revascularization in patients with ST-segment-elevation myocardial infarction (MI) reduced major adverse cardiovascular events compared with culprit-only revascularization. Inclusion was based on angiographic criteria.
Objectives: We modelled non-culprit virtual fractional flow reserve (vFFR) and investigated interactions between physiological lesion severity and the benefits of complete revascularization in COMPLETE.
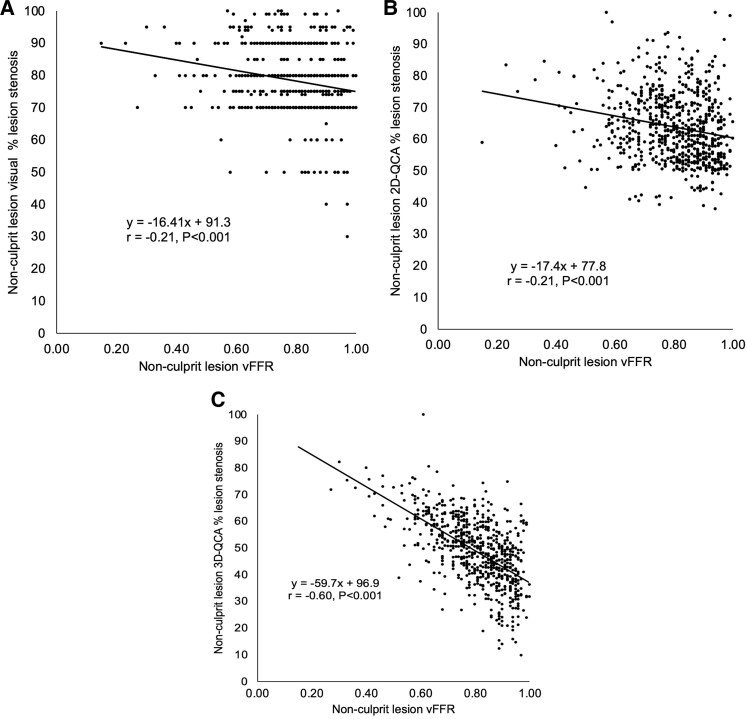
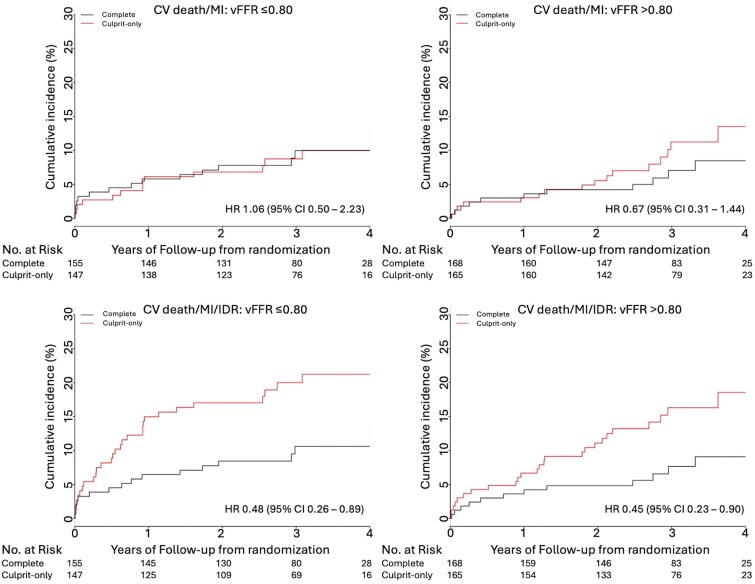
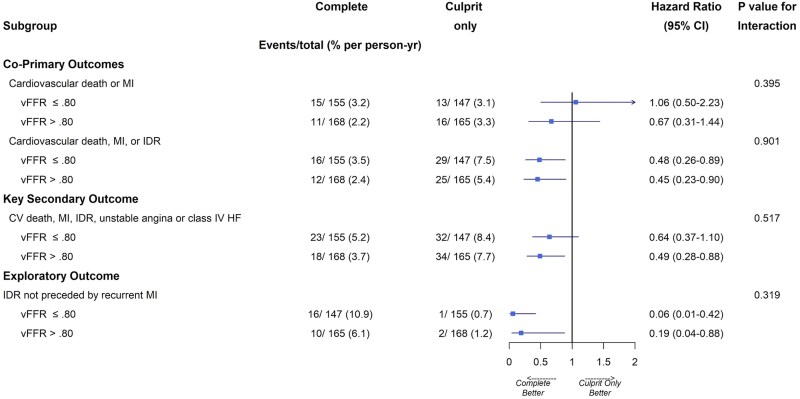
Methods and results: All suitable angiograms from COMPLETE underwent software-based 3-dimensional (3D) arterial reconstruction and analysis of 3D-quantitative coronary angiography (QCA) and vFFR using computational fluid dynamics software. Physiological lesion significance was defined as vFFR ≤0.80 and was compared with operators' visual angiographic analysis, 2D-QCA and 3D-QCA. vFFR was computed in 635 patients (710 lesions). 302 patients (48%) had ≥1 physiologically significant lesion and 333 (52%) had none. 321 (45%) lesions were physiologically significant and 389 (55%) were not. There was no statistically significant interaction between physiological lesion significance and any of the trial co-primary or key secondary clinical outcomes, or an exploratory outcome of ischaemia-driven revascularization without preceding MI (all interaction P > 0.30). 3D-QCA predicted vFFR significance more accurately than visual and 2D-QCA (concordance 73% vs. 49% vs. 59%, respectively).
Conclusion: In this virtual physiological substudy of the COMPLETE trial, 52% of patients lacked any physiologically significant lesions and the benefits of complete revascularization appeared to be independent of physiological lesion significance. 3D-QCA was a better predictor of physiological significance than either 2D-QCA or operator visual analysis. Further research is warranted to compare angiography-guided and physiology-guided complete revascularization strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


