Hoai T P Dinh, Hiroki Ushirozako, Tomohiko Hasegawa, Shigeto Ebata, Tetsuro Ohba, Hiroki Oba, Keijiro Mukaiyama, Yu Yamato, Go Yoshida, Tomohiro Banno, Hideyuki Arima, Shin Oe, Koichiro Ide, Tomohiro Yamada, Kenta Kurosu, Toshiyuki Ojima, Jun Takahashi, Hirotaka Haro, Yukihiro Matsuyama
{"title":"单节段后路或经椎间孔腰椎椎间融合术后椎笼下沉的危险因素和后果:一项回顾性多中心研究。","authors":"Hoai T P Dinh, Hiroki Ushirozako, Tomohiko Hasegawa, Shigeto Ebata, Tetsuro Ohba, Hiroki Oba, Keijiro Mukaiyama, Yu Yamato, Go Yoshida, Tomohiro Banno, Hideyuki Arima, Shin Oe, Koichiro Ide, Tomohiro Yamada, Kenta Kurosu, Toshiyuki Ojima, Jun Takahashi, Hirotaka Haro, Yukihiro Matsuyama","doi":"10.22603/ssrr.2024-0241","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cage subsidence (CS) after posterior or transforaminal lumbar interbody fusion (PLIF or TLIF) is challenging; however, its impact on health-related quality of life (HRQOL) remains unclear. This study aimed to explore the impact of CS occurrence on HRQOL and identify the risk factors in patients following PLIF or TLIF.</p><p><strong>Methods: </strong>A total of 138 patients (mean age, 67 years; follow-up period, 12 months) who underwent single-level PLIF or TLIF were retrospectively analyzed. CS was defined as >1 mm sinking of the intervertebral cage evaluated via computed tomography. The patients were divided into the CS and nonsubsidence (NS) groups. HRQOL was assessed using the Oswestry Disability Index (ODI) scores.</p><p><strong>Results: </strong>Among the 138 patients, 30 (22%) developed CS following PLIF or TLIF. All cases with TLIF surgery (n=25) involved the use of one cage. A significant difference was observed in the use of two cages between the CS and NS groups (20.0% vs. 48.1%; <i>P</i>=0.006). The CS group had lower occupancy rate of autograft soon after the operation than the NS groups (<i>P</i>=0.002), and the occupancy rate of autograft tended to decrease in the CS group compared with the NS group over time. The ODI scores improved in both groups postoperatively; however, the NS group exhibited greater improvements in ODI scores from 4 months postoperatively. The CS group had a significantly lower proportion of patients with intervertebral osseous union at 6 and 12 months postoperatively compared with the NS group (<i>P</i>=0.003 and <i>P</i><0.001, respectively).</p><p><strong>Conclusions: </strong>The use of two intervertebral cages may enhance initial stability and reduce CS risk after PLIF. Initial intervertebral stability was crucial to preventing CS occurrence, as evidenced by the high occupancy rates of autograft in patients without CS. Surgical factors, including surgical strategy and intraoperative techniques, should be considered to prevent CS occurrence and to improve surgical outcomes and patient satisfaction.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"9 3","pages":"339-349"},"PeriodicalIF":1.2000,"publicationDate":"2024-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151272/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors and Consequences of Cage Subsidence after Single-level Posterior or Transforaminal Lumbar Interbody Fusion: A Retrospective Multicenter Study.\",\"authors\":\"Hoai T P Dinh, Hiroki Ushirozako, Tomohiko Hasegawa, Shigeto Ebata, Tetsuro Ohba, Hiroki Oba, Keijiro Mukaiyama, Yu Yamato, Go Yoshida, Tomohiro Banno, Hideyuki Arima, Shin Oe, Koichiro Ide, Tomohiro Yamada, Kenta Kurosu, Toshiyuki Ojima, Jun Takahashi, Hirotaka Haro, Yukihiro Matsuyama\",\"doi\":\"10.22603/ssrr.2024-0241\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cage subsidence (CS) after posterior or transforaminal lumbar interbody fusion (PLIF or TLIF) is challenging; however, its impact on health-related quality of life (HRQOL) remains unclear. This study aimed to explore the impact of CS occurrence on HRQOL and identify the risk factors in patients following PLIF or TLIF.</p><p><strong>Methods: </strong>A total of 138 patients (mean age, 67 years; follow-up period, 12 months) who underwent single-level PLIF or TLIF were retrospectively analyzed. CS was defined as >1 mm sinking of the intervertebral cage evaluated via computed tomography. The patients were divided into the CS and nonsubsidence (NS) groups. HRQOL was assessed using the Oswestry Disability Index (ODI) scores.</p><p><strong>Results: </strong>Among the 138 patients, 30 (22%) developed CS following PLIF or TLIF. All cases with TLIF surgery (n=25) involved the use of one cage. A significant difference was observed in the use of two cages between the CS and NS groups (20.0% vs. 48.1%; <i>P</i>=0.006). The CS group had lower occupancy rate of autograft soon after the operation than the NS groups (<i>P</i>=0.002), and the occupancy rate of autograft tended to decrease in the CS group compared with the NS group over time. The ODI scores improved in both groups postoperatively; however, the NS group exhibited greater improvements in ODI scores from 4 months postoperatively. The CS group had a significantly lower proportion of patients with intervertebral osseous union at 6 and 12 months postoperatively compared with the NS group (<i>P</i>=0.003 and <i>P</i><0.001, respectively).</p><p><strong>Conclusions: </strong>The use of two intervertebral cages may enhance initial stability and reduce CS risk after PLIF. Initial intervertebral stability was crucial to preventing CS occurrence, as evidenced by the high occupancy rates of autograft in patients without CS. Surgical factors, including surgical strategy and intraoperative techniques, should be considered to prevent CS occurrence and to improve surgical outcomes and patient satisfaction.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"9 3\",\"pages\":\"339-349\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-12-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151272/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2024-0241\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/27 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0241","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
后路或经椎间孔腰椎椎间融合术(PLIF或tliff)后的椎笼沉降(CS)是具有挑战性的;然而,其对健康相关生活质量(HRQOL)的影响尚不清楚。本研究旨在探讨CS发生对PLIF或TLIF患者HRQOL的影响,并确定其危险因素。方法:共138例患者(平均年龄67岁;回顾性分析接受单节段PLIF或TLIF的患者。CS定义为通过计算机断层扫描评估椎间笼下沉>.1 mm。将患者分为CS组和不沉降(NS)组。HRQOL采用Oswestry残疾指数(ODI)评分进行评估。结果:138例患者中,30例(22%)在PLIF或TLIF后发生CS。所有TLIF手术病例(n=25)均使用一个笼。CS组和NS组在两种笼的使用上有显著差异(20.0% vs 48.1%;P = 0.006)。CS组术后不久自体移植物占位率低于NS组(P=0.002),且随时间推移CS组自体移植物占位率较NS组有降低的趋势。两组患者术后ODI评分均有改善;然而,NS组术后4个月ODI评分有较大改善。与NS组相比,CS组术后6个月和12个月椎间骨愈合的患者比例显著降低(P=0.003和P)。结论:使用两个椎间笼可以增强PLIF术后的初始稳定性,降低CS风险。最初的椎间稳定对于预防CS的发生至关重要,无CS患者自体移植物的高占位率证明了这一点。应考虑手术策略和术中技术等手术因素,以预防CS的发生,提高手术效果和患者满意度。
Risk Factors and Consequences of Cage Subsidence after Single-level Posterior or Transforaminal Lumbar Interbody Fusion: A Retrospective Multicenter Study.
Introduction: Cage subsidence (CS) after posterior or transforaminal lumbar interbody fusion (PLIF or TLIF) is challenging; however, its impact on health-related quality of life (HRQOL) remains unclear. This study aimed to explore the impact of CS occurrence on HRQOL and identify the risk factors in patients following PLIF or TLIF.
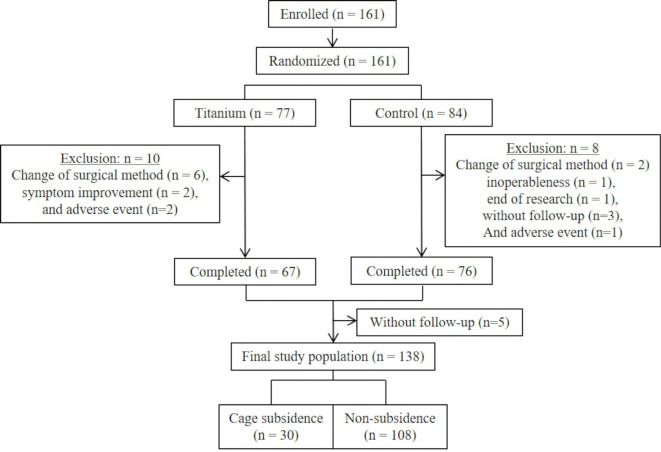
Methods: A total of 138 patients (mean age, 67 years; follow-up period, 12 months) who underwent single-level PLIF or TLIF were retrospectively analyzed. CS was defined as >1 mm sinking of the intervertebral cage evaluated via computed tomography. The patients were divided into the CS and nonsubsidence (NS) groups. HRQOL was assessed using the Oswestry Disability Index (ODI) scores.
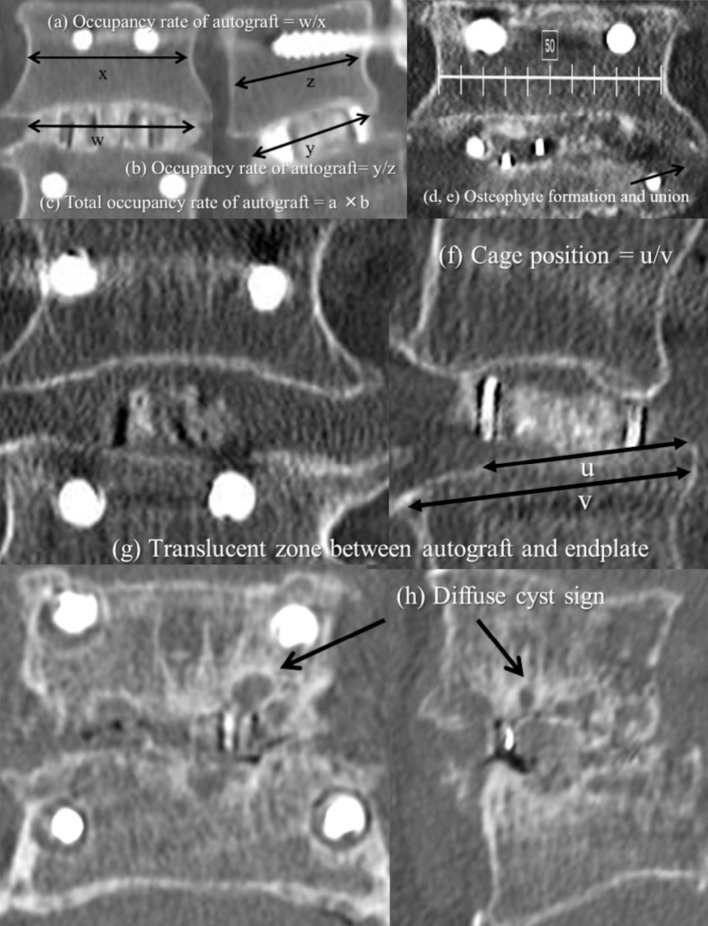
Results: Among the 138 patients, 30 (22%) developed CS following PLIF or TLIF. All cases with TLIF surgery (n=25) involved the use of one cage. A significant difference was observed in the use of two cages between the CS and NS groups (20.0% vs. 48.1%; P=0.006). The CS group had lower occupancy rate of autograft soon after the operation than the NS groups (P=0.002), and the occupancy rate of autograft tended to decrease in the CS group compared with the NS group over time. The ODI scores improved in both groups postoperatively; however, the NS group exhibited greater improvements in ODI scores from 4 months postoperatively. The CS group had a significantly lower proportion of patients with intervertebral osseous union at 6 and 12 months postoperatively compared with the NS group (P=0.003 and P<0.001, respectively).
Conclusions: The use of two intervertebral cages may enhance initial stability and reduce CS risk after PLIF. Initial intervertebral stability was crucial to preventing CS occurrence, as evidenced by the high occupancy rates of autograft in patients without CS. Surgical factors, including surgical strategy and intraoperative techniques, should be considered to prevent CS occurrence and to improve surgical outcomes and patient satisfaction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


