{"title":"贲门失弛缓症相关肠系膜上动脉综合征伴胃扩张。","authors":"Zaim Gashi, Leutrim Shabani, Endrit Shatrolli","doi":"10.12890/2025_005461","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Achalasia and superior mesenteric artery (SMA) syndrome are both uncommon gastrointestinal disorders. When they occur together-a rare clinical scenario-they can cause serious complications, including severe gastric distension.</p><p><strong>Case presentation: </strong>We report the case of a 62-year-old man with a known history of achalasia, previously managed with botulinum toxin injections. He presented with progressively worsening abdominal bloating, unintentional weight loss, and abdominal discomfort. Endoscopy revealed a strikingly dilated oesophagus and stomach, filled with nearly 9 litres of fluid. Further imaging with computed tomography angiography showed a narrowed aortomesenteric angle measuring just 16.7°, consistent with a diagnosis of SMA syndrome. Remarkably, despite the massive distension, no perforation was identified.</p><p><strong>Discussion: </strong>This case highlights a rare but important overlap between achalasia and SMA syndrome, leading to extreme gastric dilatation in the absence of rupture. Despite the extreme degree of gastric dilatation observed on both endoscopy and imaging, the stomach wall remained intact, and there were no signs of ischemia or perforation. Although SMA syndrome may occur secondary to other health conditions, this case underscores how variable and potentially dangerous this dual pathology can be.</p><p><strong>Conclusion: </strong>Clinicians should remain vigilant for the possibility of SMA syndrome in patients with achalasia who develop new or worsening upper gastrointestinal symptoms, particularly if there is significant gastric dilatation. Early imaging and recognition can be crucial in preventing severe outcomes like perforation.</p><p><strong>Learning points: </strong>The patient has a very rare combination of achalasia and superior mesenteric artery syndrome, presenting with massive dilatation of the stomach with no perforation.Early detection through computed tomography angiography and early decompression are essential to prevent potentially fatal complications, including gastric rupture.This case adds to the limited literature describing achalasia-superior mesenteric artery overlap and reinforces the need for a high degree of clinical suspicion when symptoms diverge from baseline.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 6","pages":"005461"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151572/pdf/","citationCount":"0","resultStr":"{\"title\":\"Achalasia-Associated Superior Mesenteric Artery Syndrome with Massive Gastric Dilatation.\",\"authors\":\"Zaim Gashi, Leutrim Shabani, Endrit Shatrolli\",\"doi\":\"10.12890/2025_005461\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Achalasia and superior mesenteric artery (SMA) syndrome are both uncommon gastrointestinal disorders. When they occur together-a rare clinical scenario-they can cause serious complications, including severe gastric distension.</p><p><strong>Case presentation: </strong>We report the case of a 62-year-old man with a known history of achalasia, previously managed with botulinum toxin injections. He presented with progressively worsening abdominal bloating, unintentional weight loss, and abdominal discomfort. Endoscopy revealed a strikingly dilated oesophagus and stomach, filled with nearly 9 litres of fluid. Further imaging with computed tomography angiography showed a narrowed aortomesenteric angle measuring just 16.7°, consistent with a diagnosis of SMA syndrome. Remarkably, despite the massive distension, no perforation was identified.</p><p><strong>Discussion: </strong>This case highlights a rare but important overlap between achalasia and SMA syndrome, leading to extreme gastric dilatation in the absence of rupture. Despite the extreme degree of gastric dilatation observed on both endoscopy and imaging, the stomach wall remained intact, and there were no signs of ischemia or perforation. Although SMA syndrome may occur secondary to other health conditions, this case underscores how variable and potentially dangerous this dual pathology can be.</p><p><strong>Conclusion: </strong>Clinicians should remain vigilant for the possibility of SMA syndrome in patients with achalasia who develop new or worsening upper gastrointestinal symptoms, particularly if there is significant gastric dilatation. Early imaging and recognition can be crucial in preventing severe outcomes like perforation.</p><p><strong>Learning points: </strong>The patient has a very rare combination of achalasia and superior mesenteric artery syndrome, presenting with massive dilatation of the stomach with no perforation.Early detection through computed tomography angiography and early decompression are essential to prevent potentially fatal complications, including gastric rupture.This case adds to the limited literature describing achalasia-superior mesenteric artery overlap and reinforces the need for a high degree of clinical suspicion when symptoms diverge from baseline.</p>\",\"PeriodicalId\":11908,\"journal\":{\"name\":\"European journal of case reports in internal medicine\",\"volume\":\"12 6\",\"pages\":\"005461\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151572/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of case reports in internal medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12890/2025_005461\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005461","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Achalasia-Associated Superior Mesenteric Artery Syndrome with Massive Gastric Dilatation.
Background: Achalasia and superior mesenteric artery (SMA) syndrome are both uncommon gastrointestinal disorders. When they occur together-a rare clinical scenario-they can cause serious complications, including severe gastric distension.
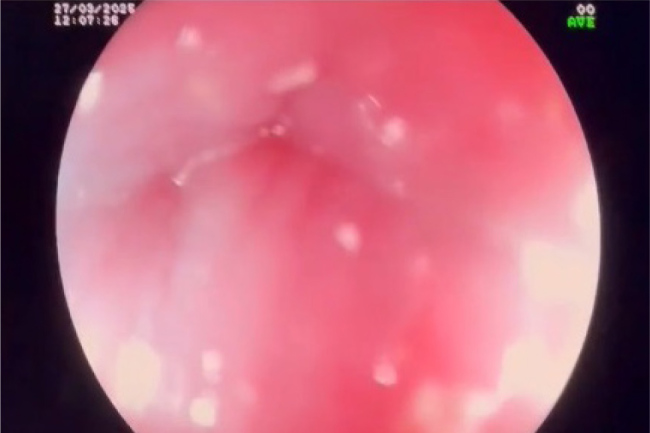
Case presentation: We report the case of a 62-year-old man with a known history of achalasia, previously managed with botulinum toxin injections. He presented with progressively worsening abdominal bloating, unintentional weight loss, and abdominal discomfort. Endoscopy revealed a strikingly dilated oesophagus and stomach, filled with nearly 9 litres of fluid. Further imaging with computed tomography angiography showed a narrowed aortomesenteric angle measuring just 16.7°, consistent with a diagnosis of SMA syndrome. Remarkably, despite the massive distension, no perforation was identified.
Discussion: This case highlights a rare but important overlap between achalasia and SMA syndrome, leading to extreme gastric dilatation in the absence of rupture. Despite the extreme degree of gastric dilatation observed on both endoscopy and imaging, the stomach wall remained intact, and there were no signs of ischemia or perforation. Although SMA syndrome may occur secondary to other health conditions, this case underscores how variable and potentially dangerous this dual pathology can be.
Conclusion: Clinicians should remain vigilant for the possibility of SMA syndrome in patients with achalasia who develop new or worsening upper gastrointestinal symptoms, particularly if there is significant gastric dilatation. Early imaging and recognition can be crucial in preventing severe outcomes like perforation.
Learning points: The patient has a very rare combination of achalasia and superior mesenteric artery syndrome, presenting with massive dilatation of the stomach with no perforation.Early detection through computed tomography angiography and early decompression are essential to prevent potentially fatal complications, including gastric rupture.This case adds to the limited literature describing achalasia-superior mesenteric artery overlap and reinforces the need for a high degree of clinical suspicion when symptoms diverge from baseline.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


