Lan Zhu, Zichen Zhao, Attilio Di Spiezio Sardo, Maribel Acién, Joel Naftalin, Thierry Van den Bosch, Charleen Sze-Yan Cheung, Dabao Xu, Xiaowu Huang, Grigoris Grimbizis
{"title":"附件空化子宫畸形的中欧共识*,†。","authors":"Lan Zhu, Zichen Zhao, Attilio Di Spiezio Sardo, Maribel Acién, Joel Naftalin, Thierry Van den Bosch, Charleen Sze-Yan Cheung, Dabao Xu, Xiaowu Huang, Grigoris Grimbizis","doi":"10.52054/FVVO.2025.62","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accessory cavitated uterine malformations (ACUMs) are a rare obstructive uterine anomaly that remains poorly understood, posing challenges for clinical management. The aetiopathogenesis is hypothesised to involve the duplication and persistence of ductal Müllerian tissue usually near the round ligament attachment, potentially related to gubernaculum dysfunction. ACUM is specifically classified by Acién's system, though rare variants necessitate continued international research to refine classification frameworks.</p><p><strong>Objectives: </strong>This consensus aims to develop good clinical practice recommendations for the pathophysiology, terminology, clinical presentation, diagnosis, and treatment of ACUM.</p><p><strong>Methods: </strong>A working group consisted of Chinese and European experts, after approval from the European Society for Gynaecological Endoscopy, developed recommendations based on the best available evidence and experts' opinion.</p><p><strong>Results: </strong>Patients with ACUM present with typical symptoms such as dysmenorrhea and dyspareunia, and atypical symptoms, including gastrointestinal and generalised pelvic pain. Diagnostic criteria include isolated cavitated lesions in the anterolateral myometrium near the round ligament, lined by endometrial tissue and filled with haemorrhagic fluid, surrounded by a myometrial mantle with concentric orientation of myometrial fibres, and typically associated with a normal uterine cavity. Diagnosis is most accurately made through ultrasound and magnetic resonance imaging. Surgical excision of the ACUM is considered the definitive treatment offering near-complete symptom resolution, and minimally invasive approach should be preferred when possible. The timing of surgery and the interval before attempting pregnancy remain unclear. The mode of delivery post-surgery is individualised based on the degree of myometrial involvement.</p><p><strong>Conclusions: </strong>The current consensus summarises the existing evidence on ACUM providing good clinical practice recommendations for their management. Existing gaps in the understanding and management of ACUMs, highlight the need for further research to guide clinical decision-making.</p><p><strong>What is new?: </strong>Good clinical practice recommendations for ACUM aiming to understand and optimise their management.</p>","PeriodicalId":46400,"journal":{"name":"Facts Views and Vision in ObGyn","volume":" ","pages":"157-169"},"PeriodicalIF":1.4000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12233108/pdf/","citationCount":"0","resultStr":"{\"title\":\"Euro-Chinese consensus on accessory cavitated uterine malformation<sup>*,†</sup>.\",\"authors\":\"Lan Zhu, Zichen Zhao, Attilio Di Spiezio Sardo, Maribel Acién, Joel Naftalin, Thierry Van den Bosch, Charleen Sze-Yan Cheung, Dabao Xu, Xiaowu Huang, Grigoris Grimbizis\",\"doi\":\"10.52054/FVVO.2025.62\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Accessory cavitated uterine malformations (ACUMs) are a rare obstructive uterine anomaly that remains poorly understood, posing challenges for clinical management. The aetiopathogenesis is hypothesised to involve the duplication and persistence of ductal Müllerian tissue usually near the round ligament attachment, potentially related to gubernaculum dysfunction. ACUM is specifically classified by Acién's system, though rare variants necessitate continued international research to refine classification frameworks.</p><p><strong>Objectives: </strong>This consensus aims to develop good clinical practice recommendations for the pathophysiology, terminology, clinical presentation, diagnosis, and treatment of ACUM.</p><p><strong>Methods: </strong>A working group consisted of Chinese and European experts, after approval from the European Society for Gynaecological Endoscopy, developed recommendations based on the best available evidence and experts' opinion.</p><p><strong>Results: </strong>Patients with ACUM present with typical symptoms such as dysmenorrhea and dyspareunia, and atypical symptoms, including gastrointestinal and generalised pelvic pain. Diagnostic criteria include isolated cavitated lesions in the anterolateral myometrium near the round ligament, lined by endometrial tissue and filled with haemorrhagic fluid, surrounded by a myometrial mantle with concentric orientation of myometrial fibres, and typically associated with a normal uterine cavity. Diagnosis is most accurately made through ultrasound and magnetic resonance imaging. Surgical excision of the ACUM is considered the definitive treatment offering near-complete symptom resolution, and minimally invasive approach should be preferred when possible. The timing of surgery and the interval before attempting pregnancy remain unclear. The mode of delivery post-surgery is individualised based on the degree of myometrial involvement.</p><p><strong>Conclusions: </strong>The current consensus summarises the existing evidence on ACUM providing good clinical practice recommendations for their management. Existing gaps in the understanding and management of ACUMs, highlight the need for further research to guide clinical decision-making.</p><p><strong>What is new?: </strong>Good clinical practice recommendations for ACUM aiming to understand and optimise their management.</p>\",\"PeriodicalId\":46400,\"journal\":{\"name\":\"Facts Views and Vision in ObGyn\",\"volume\":\" \",\"pages\":\"157-169\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12233108/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Facts Views and Vision in ObGyn\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.52054/FVVO.2025.62\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Facts Views and Vision in ObGyn","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52054/FVVO.2025.62","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Euro-Chinese consensus on accessory cavitated uterine malformation*,†.
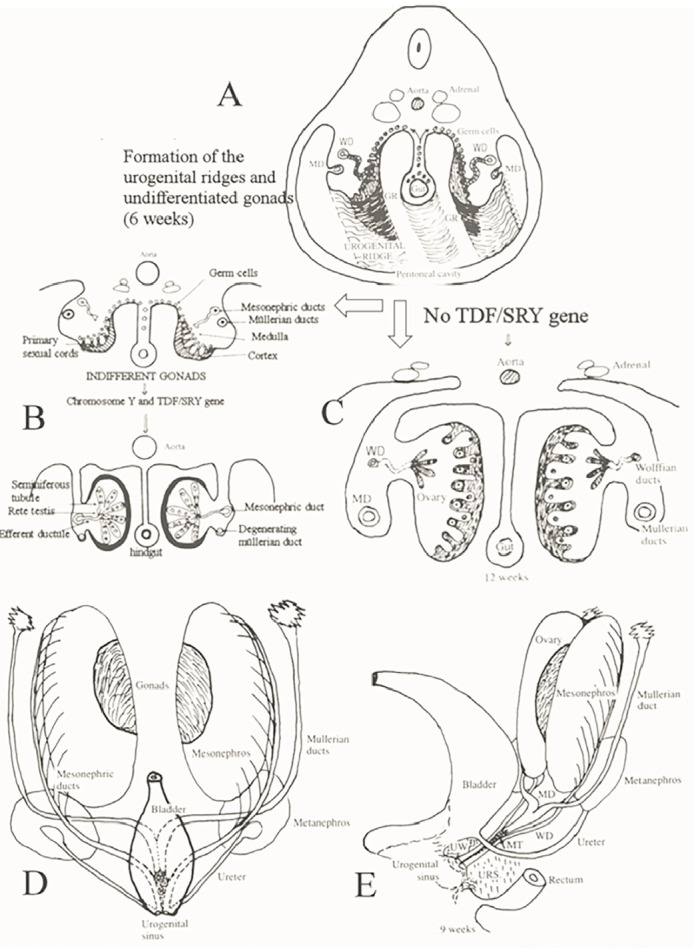
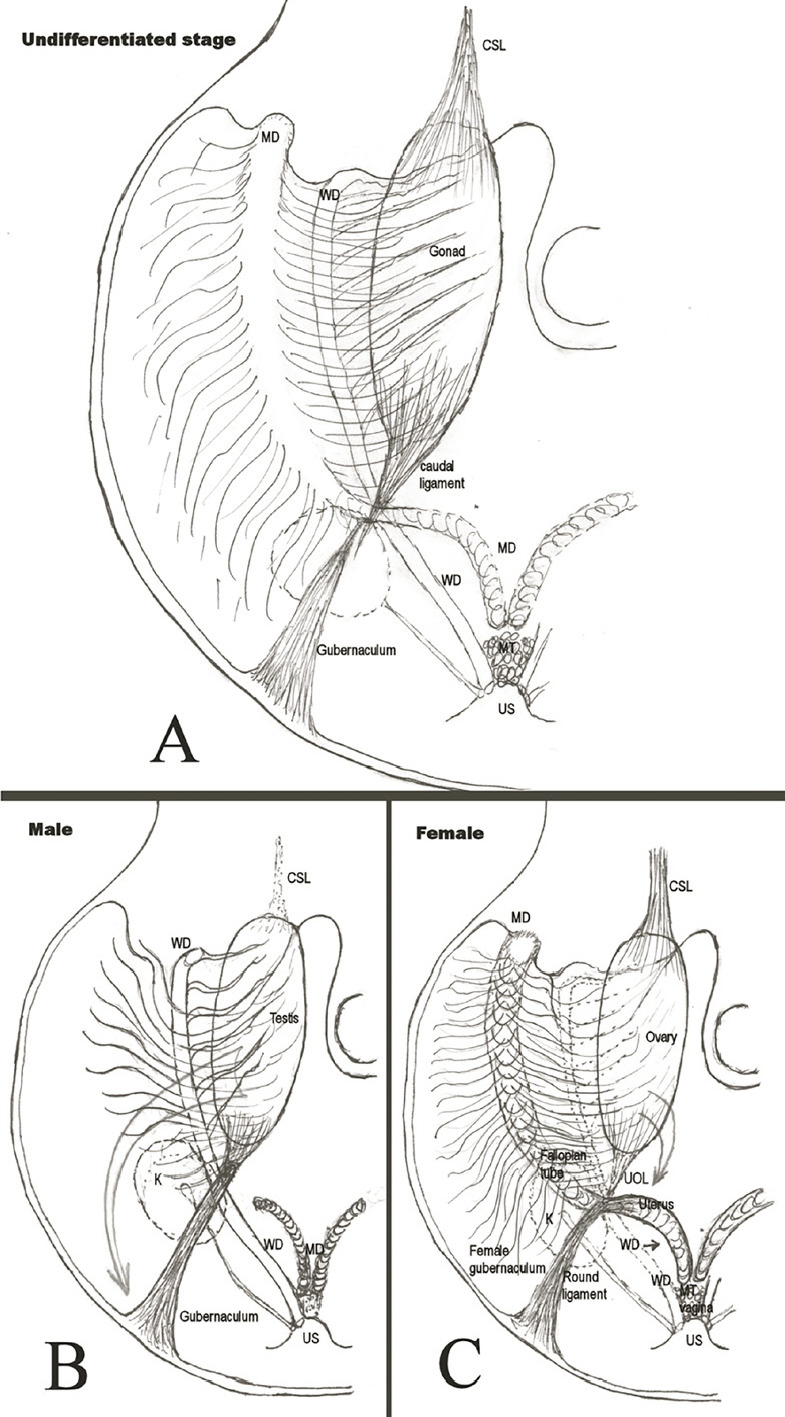
Background: Accessory cavitated uterine malformations (ACUMs) are a rare obstructive uterine anomaly that remains poorly understood, posing challenges for clinical management. The aetiopathogenesis is hypothesised to involve the duplication and persistence of ductal Müllerian tissue usually near the round ligament attachment, potentially related to gubernaculum dysfunction. ACUM is specifically classified by Acién's system, though rare variants necessitate continued international research to refine classification frameworks.
Objectives: This consensus aims to develop good clinical practice recommendations for the pathophysiology, terminology, clinical presentation, diagnosis, and treatment of ACUM.
Methods: A working group consisted of Chinese and European experts, after approval from the European Society for Gynaecological Endoscopy, developed recommendations based on the best available evidence and experts' opinion.
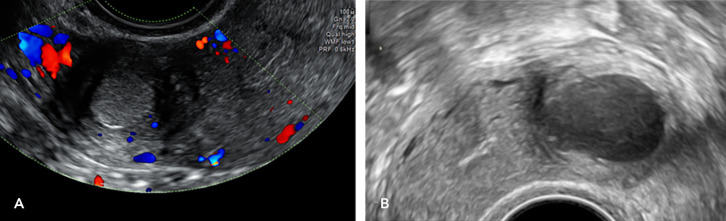
Results: Patients with ACUM present with typical symptoms such as dysmenorrhea and dyspareunia, and atypical symptoms, including gastrointestinal and generalised pelvic pain. Diagnostic criteria include isolated cavitated lesions in the anterolateral myometrium near the round ligament, lined by endometrial tissue and filled with haemorrhagic fluid, surrounded by a myometrial mantle with concentric orientation of myometrial fibres, and typically associated with a normal uterine cavity. Diagnosis is most accurately made through ultrasound and magnetic resonance imaging. Surgical excision of the ACUM is considered the definitive treatment offering near-complete symptom resolution, and minimally invasive approach should be preferred when possible. The timing of surgery and the interval before attempting pregnancy remain unclear. The mode of delivery post-surgery is individualised based on the degree of myometrial involvement.
Conclusions: The current consensus summarises the existing evidence on ACUM providing good clinical practice recommendations for their management. Existing gaps in the understanding and management of ACUMs, highlight the need for further research to guide clinical decision-making.
What is new?: Good clinical practice recommendations for ACUM aiming to understand and optimise their management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


