Alexandros A Polymeris, Masatoshi Koga, Daniel Strbian, Adhiyaman Vedamurthy, Manju Krishnan, Mattia Branca, Thomas Horvath, Martina Goeldlin, Gek Shim, Christoph Gumbinger, Liqun Zhang, Espen Saxhaug Kristoffersen, Philippe Desfontaines, Peter Vanacker, Angelika Alonso, Sven Poli, Ana Paiva Nunes, Nicoletta G Caracciolo, Markus Kneihsl, Timo Kahles, Daria Giudici, Silja Räty, Marjaana Tiainen, Jesse Dawson, Urs Fischer
{"title":"房颤相关缺血性卒中患者在开始抗凝治疗前的抗血小板使用:ELAN试验分析","authors":"Alexandros A Polymeris, Masatoshi Koga, Daniel Strbian, Adhiyaman Vedamurthy, Manju Krishnan, Mattia Branca, Thomas Horvath, Martina Goeldlin, Gek Shim, Christoph Gumbinger, Liqun Zhang, Espen Saxhaug Kristoffersen, Philippe Desfontaines, Peter Vanacker, Angelika Alonso, Sven Poli, Ana Paiva Nunes, Nicoletta G Caracciolo, Markus Kneihsl, Timo Kahles, Daria Giudici, Silja Räty, Marjaana Tiainen, Jesse Dawson, Urs Fischer","doi":"10.5853/jos.2024.04322","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Antiplatelets are often used before direct oral anticoagulant (DOACs) initiation after an acute ischemic stroke related to atrial fibrillation (AF), but the evidence is weak. Here, we explored the risks and benefits of this approach.</p><p><strong>Methods: </strong>A post-hoc analysis of ELAN (Early versus Late Initiation of Direct Oral Anticoagulants in Post-ischemic Stroke Patients with Atrial Fibrillation) trial data (NCT03148457) was conducted to compare the risk of recurrent ischemic stroke, systemic embolism, major bleeding (extracranial or intracranial hemorrhage [ICH]), and vascular death within 30 days (as a composite and as individual outcomes) in participants treated with and without antiplatelets before DOAC initiation after an AF-associated ischemic stroke. We used both logistic and cause-specific Cox proportional hazards regression in inverse probability of treatment weighted models to account for confounding. We calculated the net benefit of antiplatelet use by subtracting the weighted rate of excess bleeding events attributable to antiplatelets from the rate of excess ischemic events possibly prevented by antiplatelets.</p><p><strong>Results: </strong>Among 2,013 participants (median age 77 years, 45.5% female), 1,090 (54.1%) used antiplatelets, and 70 (3.5%) experienced the composite outcome. Antiplatelet use was not associated with the composite outcome (inverse probability of treatment weighted odds ratio [ORweighted] 1.06, 95% confidence interval [CI] 0.66-1.72; inverse probability of treatment weighted hazard ratio [HRweighted] 1.06, 95% CI 0.65-1.72), but showed a lower risk of ischemic stroke recurrence (ORweighted 0.58 [0.30-1.08], HRweighted 0.57 [0.30-1.10]), and a higher risk of major bleeding (ORweighted 1.76 [0.56-6.63], HRweighted 1.88 [0.56-6.39]). Its net benefit was +0.57 (95% CI -1.25 to +2.34) to +0.30 (-1.82 to +2.27) weighted events/100 person-months for ICH weights 1.5 to 3.1.</p><p><strong>Conclusion: </strong>Following an AF-associated ischemic stroke, we found a lower risk of recurrence and no signs of net harm with antiplatelet use before DOAC initiation, despite an increased risk of bleeding.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"27 2","pages":"217-227"},"PeriodicalIF":8.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152450/pdf/","citationCount":"0","resultStr":"{\"title\":\"Antiplatelet Use Prior to Anticoagulant Initiation in Patients With Atrial Fibrillation-Related Ischemic Stroke: An ELAN Trial Analysis.\",\"authors\":\"Alexandros A Polymeris, Masatoshi Koga, Daniel Strbian, Adhiyaman Vedamurthy, Manju Krishnan, Mattia Branca, Thomas Horvath, Martina Goeldlin, Gek Shim, Christoph Gumbinger, Liqun Zhang, Espen Saxhaug Kristoffersen, Philippe Desfontaines, Peter Vanacker, Angelika Alonso, Sven Poli, Ana Paiva Nunes, Nicoletta G Caracciolo, Markus Kneihsl, Timo Kahles, Daria Giudici, Silja Räty, Marjaana Tiainen, Jesse Dawson, Urs Fischer\",\"doi\":\"10.5853/jos.2024.04322\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Antiplatelets are often used before direct oral anticoagulant (DOACs) initiation after an acute ischemic stroke related to atrial fibrillation (AF), but the evidence is weak. Here, we explored the risks and benefits of this approach.</p><p><strong>Methods: </strong>A post-hoc analysis of ELAN (Early versus Late Initiation of Direct Oral Anticoagulants in Post-ischemic Stroke Patients with Atrial Fibrillation) trial data (NCT03148457) was conducted to compare the risk of recurrent ischemic stroke, systemic embolism, major bleeding (extracranial or intracranial hemorrhage [ICH]), and vascular death within 30 days (as a composite and as individual outcomes) in participants treated with and without antiplatelets before DOAC initiation after an AF-associated ischemic stroke. We used both logistic and cause-specific Cox proportional hazards regression in inverse probability of treatment weighted models to account for confounding. We calculated the net benefit of antiplatelet use by subtracting the weighted rate of excess bleeding events attributable to antiplatelets from the rate of excess ischemic events possibly prevented by antiplatelets.</p><p><strong>Results: </strong>Among 2,013 participants (median age 77 years, 45.5% female), 1,090 (54.1%) used antiplatelets, and 70 (3.5%) experienced the composite outcome. Antiplatelet use was not associated with the composite outcome (inverse probability of treatment weighted odds ratio [ORweighted] 1.06, 95% confidence interval [CI] 0.66-1.72; inverse probability of treatment weighted hazard ratio [HRweighted] 1.06, 95% CI 0.65-1.72), but showed a lower risk of ischemic stroke recurrence (ORweighted 0.58 [0.30-1.08], HRweighted 0.57 [0.30-1.10]), and a higher risk of major bleeding (ORweighted 1.76 [0.56-6.63], HRweighted 1.88 [0.56-6.39]). Its net benefit was +0.57 (95% CI -1.25 to +2.34) to +0.30 (-1.82 to +2.27) weighted events/100 person-months for ICH weights 1.5 to 3.1.</p><p><strong>Conclusion: </strong>Following an AF-associated ischemic stroke, we found a lower risk of recurrence and no signs of net harm with antiplatelet use before DOAC initiation, despite an increased risk of bleeding.</p>\",\"PeriodicalId\":17135,\"journal\":{\"name\":\"Journal of Stroke\",\"volume\":\"27 2\",\"pages\":\"217-227\"},\"PeriodicalIF\":8.6000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12152450/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Stroke\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5853/jos.2024.04322\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2024.04322","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:心房颤动(AF)相关急性缺血性卒中后,抗血小板常在直接口服抗凝剂(DOACs)开始前使用,但证据不足。在这里,我们探讨了这种方法的风险和好处。方法:对ELAN(缺血性卒中后心房颤动患者早期与晚期直接口服抗凝剂)试验数据(NCT03148457)进行事后分析,比较缺血性卒中复发、全身性栓塞、大出血(颅外或颅内出血[ICH])的风险。af相关缺血性卒中患者在DOAC开始前接受或未接受抗血小板治疗的30天内血管死亡(作为综合和个体结果)。我们在处理加权模型的逆概率中使用逻辑回归和原因特异性Cox比例风险回归来解释混淆。我们通过从抗血小板可能预防的过量缺血事件的比率中减去由抗血小板引起的过量出血事件的加权比率来计算抗血小板使用的净收益。结果:在2013名参与者中(中位年龄77岁,45.5%为女性),1090名(54.1%)使用抗血小板药物,70名(3.5%)经历了复合结局。抗血小板使用与综合结果无关(治疗加权比值比(or加权)为1.06,95%可信区间[CI] 0.66-1.72;治疗加权风险比的负概率[hr加权]1.06,95% CI 0.65-1.72),但缺血性卒中复发风险较低(or加权0.58 [0.30-1.08],hr加权0.57[0.30-1.10]),大出血风险较高(or加权1.76 [0.56-6.63],hr加权1.88[0.56-6.39])。对于ICH权重为1.5至3.1的患者,其净获益为+0.57 (95% CI -1.25至+2.34)至+0.30(-1.82至+2.27)加权事件/100人月。结论:在房颤相关的缺血性卒中后,我们发现在DOAC开始前使用抗血小板可降低复发风险,且无净伤害迹象,尽管出血风险增加。
Antiplatelet Use Prior to Anticoagulant Initiation in Patients With Atrial Fibrillation-Related Ischemic Stroke: An ELAN Trial Analysis.
Background and purpose: Antiplatelets are often used before direct oral anticoagulant (DOACs) initiation after an acute ischemic stroke related to atrial fibrillation (AF), but the evidence is weak. Here, we explored the risks and benefits of this approach.
Methods: A post-hoc analysis of ELAN (Early versus Late Initiation of Direct Oral Anticoagulants in Post-ischemic Stroke Patients with Atrial Fibrillation) trial data (NCT03148457) was conducted to compare the risk of recurrent ischemic stroke, systemic embolism, major bleeding (extracranial or intracranial hemorrhage [ICH]), and vascular death within 30 days (as a composite and as individual outcomes) in participants treated with and without antiplatelets before DOAC initiation after an AF-associated ischemic stroke. We used both logistic and cause-specific Cox proportional hazards regression in inverse probability of treatment weighted models to account for confounding. We calculated the net benefit of antiplatelet use by subtracting the weighted rate of excess bleeding events attributable to antiplatelets from the rate of excess ischemic events possibly prevented by antiplatelets.
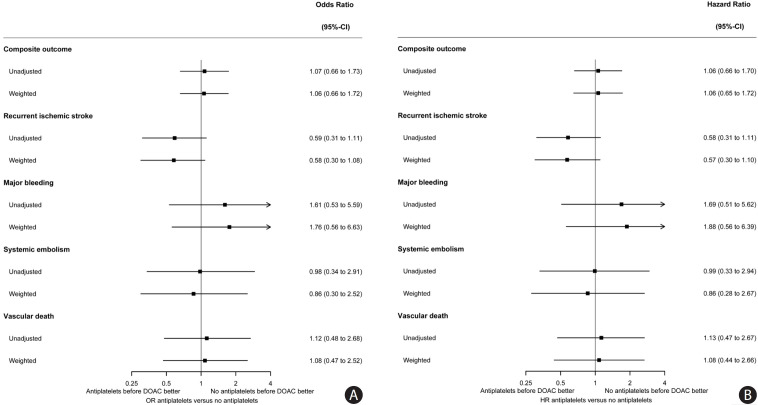
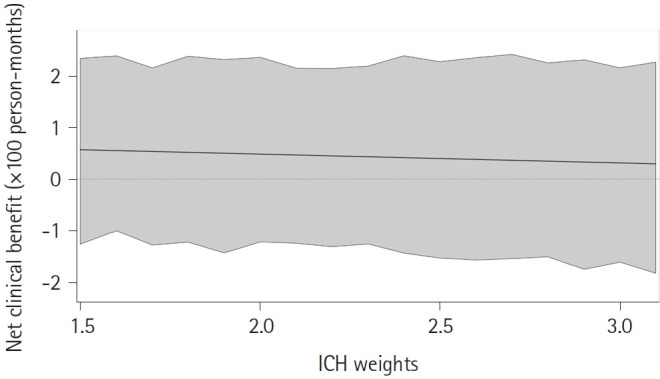
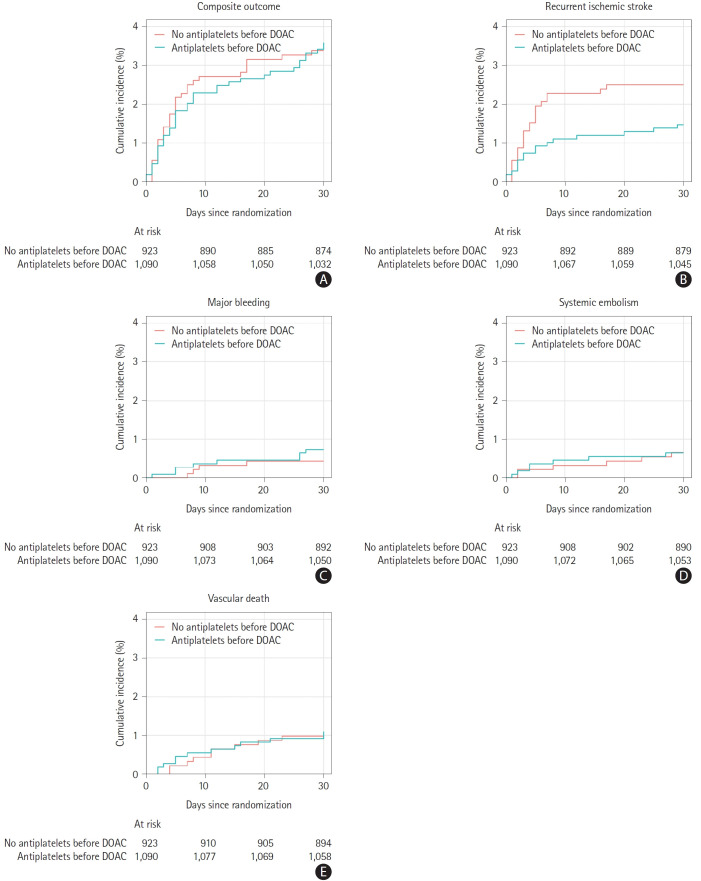
Results: Among 2,013 participants (median age 77 years, 45.5% female), 1,090 (54.1%) used antiplatelets, and 70 (3.5%) experienced the composite outcome. Antiplatelet use was not associated with the composite outcome (inverse probability of treatment weighted odds ratio [ORweighted] 1.06, 95% confidence interval [CI] 0.66-1.72; inverse probability of treatment weighted hazard ratio [HRweighted] 1.06, 95% CI 0.65-1.72), but showed a lower risk of ischemic stroke recurrence (ORweighted 0.58 [0.30-1.08], HRweighted 0.57 [0.30-1.10]), and a higher risk of major bleeding (ORweighted 1.76 [0.56-6.63], HRweighted 1.88 [0.56-6.39]). Its net benefit was +0.57 (95% CI -1.25 to +2.34) to +0.30 (-1.82 to +2.27) weighted events/100 person-months for ICH weights 1.5 to 3.1.
Conclusion: Following an AF-associated ischemic stroke, we found a lower risk of recurrence and no signs of net harm with antiplatelet use before DOAC initiation, despite an increased risk of bleeding.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


