外窥镜眶上锁眼入路治疗颅底病变:一个机构经验。
摘要
近年来,与传统的翼点和额颞部入路相比,经眉部切口的眶上入路在针对前颅底和少数中颅窝病变方面得到了广泛的应用。然而,通过这种方法极其狭窄的视角需要经常调整手术台和显微镜以获得最佳的可视化。在如此深的位置通过如此小的开口照明是另一个限制因素。考虑到这些问题和显微镜的笨重,经验丰富的外科医生逐渐转向纯内窥镜或内窥镜辅助下的眶上锁孔入路。但由于成本高,学习曲线陡峭,以及在充满血液的腔中面临的困难,它也受到限制。为了规避显微镜和内窥镜的这些限制,眶上锁孔入路可以通过外窥镜(ExSOKHA)完成。尽管使用外窥镜的各种颅骨手术在当代已经很好地建立起来,但专门针对这种仅使用外窥镜的微创眶上锁孔入路的研究和文献却很缺乏。在这里,我们的目的是研究外窥镜通过眶上锁孔入路靶向颅底病变的可行性和实用性,以确定它是否可以用于从显微镜到内窥镜过渡的学习,主要目标是外窥镜在SOKHA技术中的用户友好性。材料与方法本前瞻性观察研究在神经外科进行,为期7年。样本量为50。该研究使用了外窥镜和支撑臂- 2d VITOM刚性透镜望远镜(型号28095 VA, Karl Storz内窥镜,德国图特林根),外径10毫米,轴长14厘米,光源(Xenon Nova 300, Karl Storz GmBH and Co,德国图特林根),摄像机头,视频显示器和握臂。结果50例患者中以垂体腺瘤(30%)和脑膜瘤(38%)居多,动脉瘤占6%;仅4例(8%)发生误开额窦,2例(4%)发生术后脑脊液漏。手术时间为2 ~ 4小时,其中动脉瘤夹闭/脑脊液鼻漏最短,脑膜瘤和垂体腺瘤切除最长。术中,外窥镜重新定位调整最多需要9次,这大大减少了整体手术时间。近全切除8例;剩余的肿瘤完全切除,动脉瘤完全夹闭。住院时间为4 ~ 7天,平均重症监护病房(ICU)住院时间为3天。所有患者均无任何外科整形畸形。所有患者的格拉斯哥预后评分均为良好(4/5或5/5)。因此,ExSOKHA在手术时间、调整频率、切除和夹持的完全性以及复发方面都取得了良好的效果。其他参数,如无意的额窦侵犯、术后脑脊液泄漏、住院时间、外观畸形和预后,结果也具有可同性。结论外窥镜是望远系统的进一步发展,它提供了更大的焦距(250-550 mm),符合人体工程学的手术效果,对经眶上锁孔入路的颅底病变提供了更好的深度照明,由于增加了角能见度和易于操作,大大缩短了手术时间,提高了切除边缘。它有助于学习神经内窥镜与熟悉的原理微神经外科,可能缩短学习曲线。它在内窥镜和显微镜之间架起了桥梁,因为手术是在看屏幕的同时进行的(就像在内窥镜中一样),但不需要把镜放在手术区域内(就像在显微镜中一样),这使得它更容易操作,同时也限制了空间的占用。

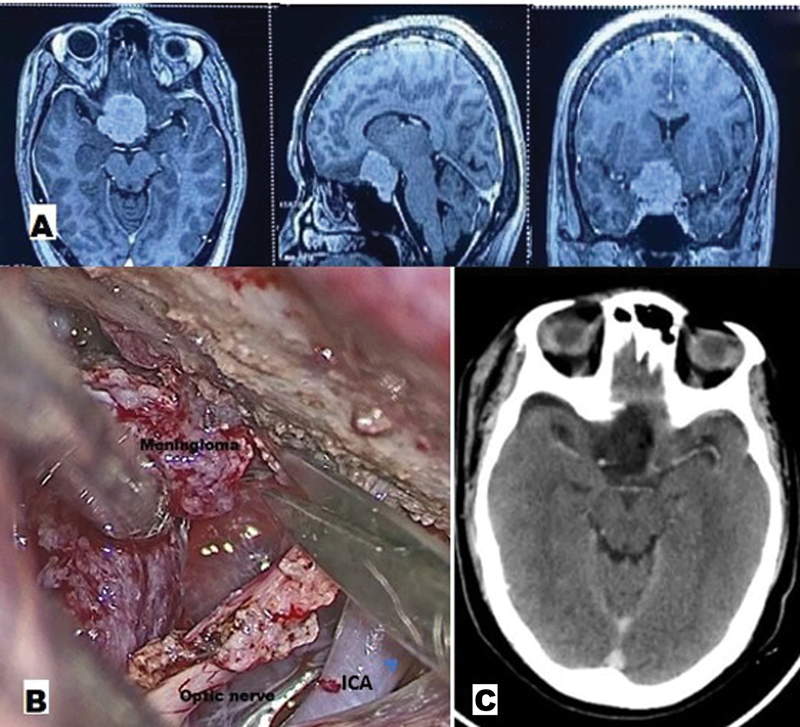
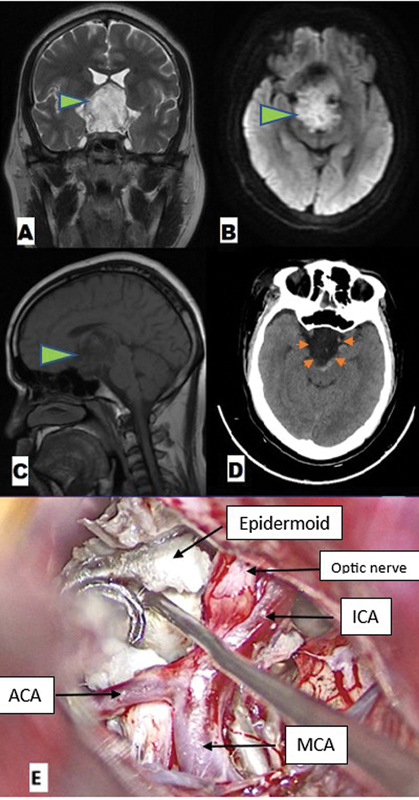
Background In recent times, the supraorbital approach via eyebrow incision has gained tremendous popularity in targeting the anterior skull base and few middle cranial fossa lesions, over the more traditional pterional and frontotemporal approaches. However, the extremely narrow viewing angle through this approach requires frequent adjustments of the operating table and microscope for optimal visualization. Illumination via such a small opening in such deep-seated location was another limiting factor. Keeping these problems and cumbersomeness of microscope in mind, experienced surgeons gradually shifted over to purely endoscopic or endoscope-assisted supraorbital keyhole approaches. But it was also limited due to high cost, steep learning curve, and difficulties faced in blood-filled cavities. To circumvent these limitations of the microscope and endoscope, the supraorbital keyhole approach can be accomplished with an exoscope (ExSOKHA). Although various cranial procedures using exoscope have become well established in contemporary times, there is paucity of studies and literature dedicated specifically to this minimally invasive supraorbital keyhole approach using the exoscope only. Here, we aim to study the feasibility and usefulness of the exoscope in targeting skull base lesions via the supraorbital keyhole approach to determine if it can be used in learning while transitioning from the microscope to the endoscope, with the primary objective being the user friendliness of the exoscope in the SOKHA technique. Materials and Methods This prospective observational study was conducted in the department of neurosurgery over a period of 7 years. The sample size was 50. The study utilized an exoscope and support arm-2D VITOM rigid-lens telescope (Model 28095 VA, Karl Storz Endoscopy, Tuttlingen, Germany) with a 10-mm outer diameter and a shaft length of 14 cm, light source (Xenon Nova 300, Karl Storz GmBH and Co., Tuttlingen, Germany), camera head, video display monitor, and a holding arm. Results Out of 50 cases, the majority were pituitary adenomas (30%) and meningiomas (38%), with aneurysms comprising 6%; only 4 cases (8%) had inadvertent frontal sinus opening and 2 cases (4%) had postoperative cerebrospinal fluid (CSF) leak. The duration of surgery ranged from 2 to 4 hours, with the shortest being for aneurysm clipping/CSF rhinorrhea and the longest for meningioma and pituitary adenoma excision. Intraoperatively, exoscope repositioning for adjustment was required for a maximum of nine times, which significantly reduced the overall operative time. Eight cases had near total excision; the remaining tumors had complete excision and the aneurysms had complete clipping. Hospital stay ranged from 4 to 7 days, with mean intensive care unit (ICU) stay of 3 days. None of the patients had any surgical cosmetic deformity. The Glasgow Outcome Scale of all patients was good (4/5 or 5/5). Thus, ExSOKHA offered good results in terms of operative time, frequency of adjustments, completeness of excision and clipping, and recurrence. The results were also comparable for other parameters like inadvertent frontal sinus violation, postoperative CSF leak, hospital stay, cosmetic deformity, and outcome. Conclusion The exoscope is a further advancement in the telescopic system, which provides a higher focal length (250-550 mm), ergonomically superior surgery with better depth illumination in skull base lesions approached via the supraorbital keyhole approach, significantly reducing operative time and improving resection margins due to increased corner visibility and easy maneuverability. It helps learn neuroendoscopy with the familiar principles of microneurosurgery, possibly shortening the learning curves. It bridges the gap between the endoscope and the microscope as the surgery is performed while viewing the screen (as in endoscope), but without needing to take the scope inside the operative field (as in microscope), making it easier to maneuver while also limiting space occupancy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


